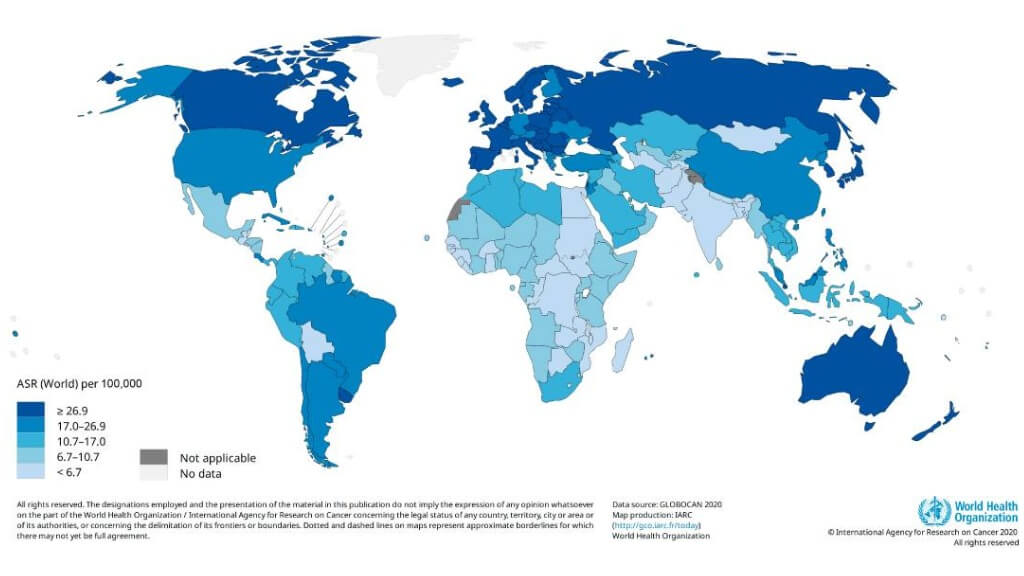
Colorectal cancer (CRC) is a major public health concern in Germany and is among the most frequently diagnosed cancers. In 2022, approximately 24,650 women and 29,960 men were newly diagnosed with CRC. Most cases arise in the colon, with relatively few in the rectum, and incidence rates increase sharply after the age of 55 years [1]. Despite significant advances in diagnostics and standard therapies, CRC remains a leading cause of cancer-related mortality.
The 5-year survival rates of colorectal cancer patients vary greatly depending on the stage of the disease一approximately 90% for early growth and only 12% for advanced tumors. These statistical data underline the need for more effective and more individualized therapies, particularly in advanced cancer patients.
Germany has become a world leader in oncology, especially in the field of immunotherapy for colorectal tumors. German clinics successfully combine immunotherapy, targeted therapy, and other measures in a modern way to increase the immune response against the tumor cells. So much more interesting and more important, however, is the fact that good percentage remission rates of over 90% for early colon and rectal tumors and about 80% for advanced colorectal malignancies have been achieved with dendritic cell vaccines in a multimodal treatment. These results suggest the great potential of modern immunotherapeutic methods for improving the course of the tumor in patients and for better tumor control.
Understanding Colon Cancer and the Role of Immunotherapy
Colorectal cancer includes malignancies arising in the colon and rectum—two distinct yet closely related segments of the large intestine. Rectal tumors has its origin in the distal part of the large bowel, known as the rectum, where it exhibits more aggressive local behavior than colonic tumors because of the constricting effect of the pelvis anatomy. Although they share similar biological mechanisms and treatment strategies, colon and rectal cancers can differ in their pathogenesis, symptom profile, and treatment approach. A deeper understanding of these conditions helps clinicians personalize oncology protocols, select the most effective immunotherapy for colon cancer, and improve the prognosis for such patients.
The group of patients eligible for immunotherapy treatment for colon cancer consists of those with high microsatellite instability in their tumors (MSI-H). This molecular feature is determined through genetic analysis of surgical specimens removed from the digestive tract. In the human genome, four genes are responsible for repairing DNA replication errors, a critical function for normal cell division. When one or more of these genes are defective, DNA damage accumulates, leading to microsatellite instability (MSI) and the formation of malignant tumor cells. A high degree of MSI occurs in about 15% of patients with colorectal tumors and in approximately 3–4% of patients with advanced disease [3]. This group is particularly sensitive to colon cancer treatment, immunotherapy in particular, with immune checkpoint inhibitors, especially PD-1 receptor blockers. These drugs increase the activity of T-lymphocytes and other immune cells, enhancing the ability of the immune system to recognize and eliminate malignant cells.
Patients with MSI-H colon cancer should also be screened for Lynch syndrome, which is a hereditary disease, determining the high risk of tumors of various organs such as the stomach, ovaries, brain, and urinary tract [4]. In this case, a multi-modal oncology approach appears to be justified, where the treatment of colon tumors will be connected with immunotherapy for colorectal cancer protocols of other malignancies, e.g., gastric or esophageal cancers.
Recent studies have shown that the application of immunotherapy for colon cancer treatment changes the clinical criteria, especially when it is applied at earlier stages. It has been proven that the application of immunotherapy for colon cancer patients significantly increases effectiveness, as reflected in remission and survival rates [5]. In leading German oncology centers, targeted therapy, immune checkpoint inhibitors, and cancer vaccines are being applied, thus stimulating a powerful immune response. The goal of the individually selected protocols of immunotherapy for colon, rectal cancer is the improvement of T-lymphocyte activation, restraining of tumor growth, and preservation of healthy tissue.
Types of Immunotherapy for Colon Cancer
Colorectal tumor cells have also acquired numerous mechanisms for evading the body's own anti-cancer defenses. They secrete immunosuppressive substances, change the structure of the tumor microenvironment, and induce chronic inflammation, all of which weaken the immune response. The basic task of the latest immunotherapy for colon cancer is therefore to counteract these mechanisms, to restore the body to its natural defense, and to induce an immune response against malignant cells.
In German oncological institutions, various classes of new drugs are used that stimulate T and other immune cells to destroy tumor cells while protecting healthy tissues. These new therapies are particularly effective in advanced colorectal cancer and are often combined with advanced targeted therapy or standard therapy protocols to achieve the best results.

Immune Checkpoint Inhibitors for Colon Cancer
One of the greatest successes in immunotherapy for colorectal cancer has been the introduction of the immune checkpoint inhibitors. Under physiological conditions, there are checkpoint proteins, e.g., PD-1, PD-L1, or CTLA-4, which the immune system uses to keep the functions of the T-cells in check, and thus to prevent damage to the healthy cells. However, the colorectal and rectal malignant cells can use these pathways and send "false" messages, thus inhibiting the immune defense.
The checkpoint inhibitors block these inhibiting messages, which means that the T-cells and other immune cells remain active and can continue to attack the malignant cells. This reactivation of the immune defense then leads to tumor shrinkage and to improved survival rates of the patients treated for advanced colorectal cancer [6].
If immune checkpoint inhibitors are combined with chemotherapy or targeted therapy, then the immune checkpoint blockade can lead to stable remission, even in advanced stages of the disease. Thus, checkpoint inhibition is one of the most effective strategies in contemporary oncology, providing a new level of precision and efficacy in cancer therapy.
Cancer Vaccines and Dendritic Cell Therapy for Colon Cancer
Unlike traditional vaccines, which are used to prevent infectious diseases, cancer vaccines are designed to induce an immune response, enabling the immune system to recognize and eliminate neoplastic cells. In the context of immunotherapy for colorectal cancer treatment, peptide and autologous vaccines have been applied to T-cells, which are exposed to known tumor antigens to sensitize them to specifically recognize and destroy neoplastic cells [7].
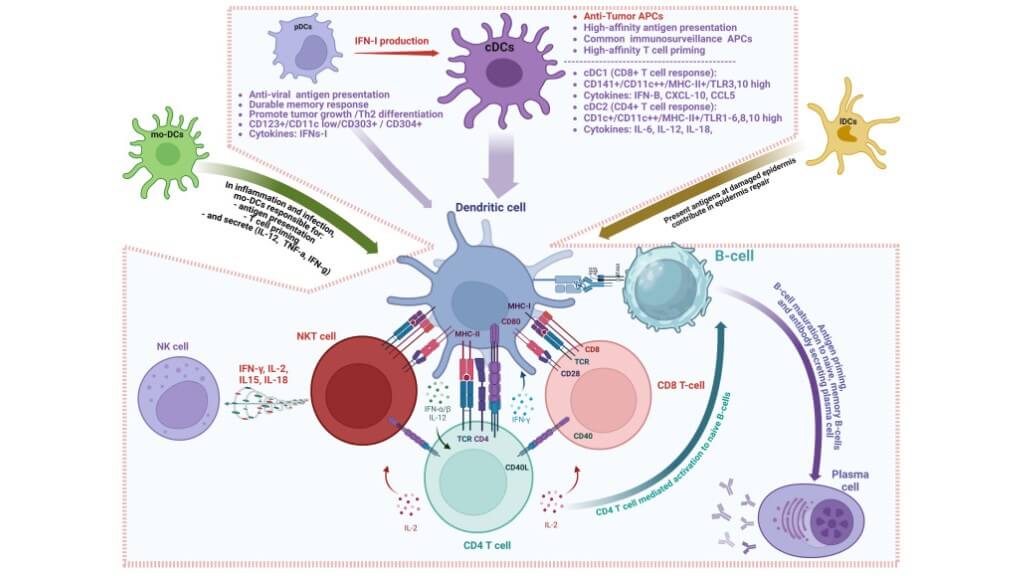
Of all vaccines, the most valuable in the therapeutic sense are the dendritic cell vaccines. These vaccines act as "teachers" of the immune system because they instruct the T-cells what targets to attack. The role that they play in the "teaching" of the immune system to initiate an anti-tumor immune response has been the subject of Nobel Prize-winning research, which emphasizes their importance.
The use of dendritic vaccines in the clinical setting has been studied in early and advanced colorectal tumors in order to improve the control over the neoplasm. These therapies increase the activity of the immune cells and raise the body’s ability to suppress neoplastic growth, while at the same time allowing the normal cells to be undisturbed. This makes the dendritic cell vaccine a promising immunotherapy for colon cancer.
The vaccines for colon cancer are:
- Autologous: These vaccines, prepared using tumor material from the patient, enable the individual’s immune system to recognize the tumor’s unique antigenic profile and to mount an appropriate immune response.
- Peptide vaccines: Through reacting to defined molecular targets like carcinoembryonic antigen (CEA) and beta-hCG, these vaccines activate the T-cells and, therefore, make the therapy more selective and reduce the side effects.
Autologous DC vaccines — prepared using the patient's own tumor material — require that the antigen source is current and representative of the tumor's present molecular profile. For colorectal cancer patients who have received prior chemotherapy with FOLFOX or FOLFIRI regimens, or anti-EGFR targeted therapy, the tumor's antigen landscape at the time of vaccination may differ from what was present at initial resection, because prior treatment exerts selective pressure on tumor cell populations.
A vaccine loaded from a resection specimen obtained before those treatment lines does not reflect the tumor the patient currently has.
Booking Health's pre-treatment review assesses whether current tissue is available to serve as the antigen source, or a liquid biopsy is scheduled before protocol is confirmed.
We’re excited to share the interview with Prof. Frank Gansauge, a true leader in personalized cancer vaccination. He discusses all aspects of this innovative procedure and explains which patients can benefit from it.
VIDEO
How Dendritic Cell Therapy is Transforming Modern Cancer Treatment
Dendritic Cell Therapy
BOOK CONSULTATION
Adoptive Cell Therapy for Colon Cancer
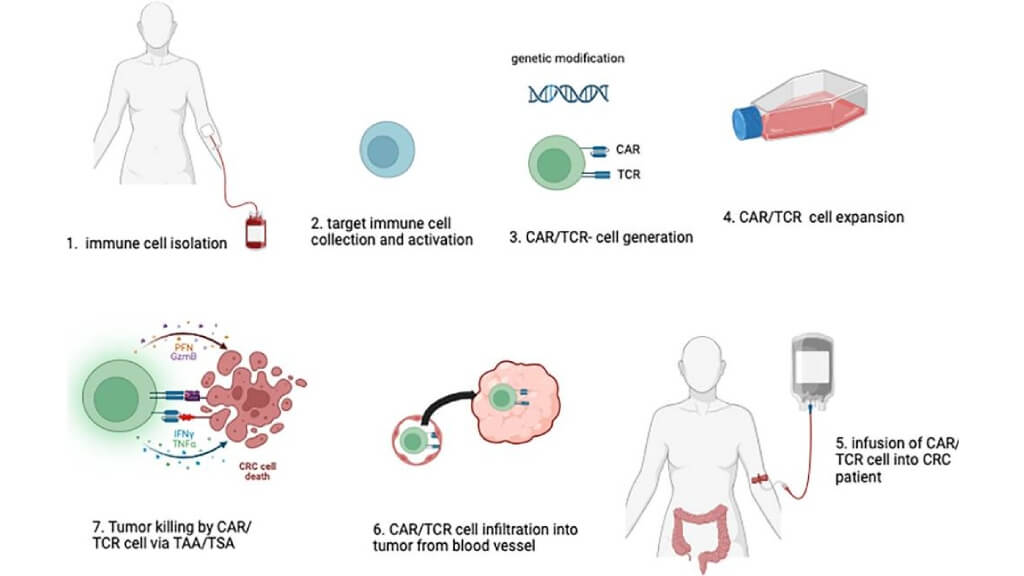
Adoptive cell therapy (ACT) is one of the most individualized forms of new immunotherapy for colon cancer in modern oncology. During the procedure, the patient’s T-cells or other immune cells are extracted from the patient's blood, genetically modified, expanded in culture, and reinfused into the body. These augmented cells act as an elite army trained to seek and destroy cancer cells that have escaped the control of the natural immune checkpoints of the body [5].
For patients with colorectal cancer with advanced disease who are no longer sensitive to standard treatments, ACT can offer a breakthrough. It increases the precision of the immune response of the organism, encourages the immune response, and gives a new hope of long-term remission.
Toll-like Receptor (TLR) Agonists
Toll-like receptors (TLRs) constitute a vital mechanism of the innate immune system, which is responsible for the detection of invading harmful agents [10]. Unfortunately, many tumor cells have found methods of escaping the detection of these receptors. TLR agonists are drugs that "wake up" the immune defense by activation of these receptors and thereafter set into play a cascade of immune modulatory processes.
Upon stimulation, immune cells secrete cytokines that recruit T-cells and enhance the immune response, leading to subsequent tumor destruction. TLR agonists are frequently used in conjunction with other methods of immunotherapy for rectal cancer, based on increased immune effectiveness, especially in patients with advanced colorectal cancer.
Emerging Immunotherapy Approaches for Colon Cancer and Colorectal Cancer
The new immunotherapy for colon cancer is aimed to provide an effective approach for not only MSI-H tumors. The modern strategies include combinations of immune checkpoint inhibitors with targeted agents (such as anti-VEGF or anti-EGFR drugs), cancer vaccines designed to stimulate tumor-specific immune responses, and adoptive cell therapies like tumor-infiltrating lymphocytes (TILs). This creates targeted immunotherapy for colon cancer that focuses on expanding treatment to microsatellite stable (MSS) tumors and improving neoadjuvant options.
When considering new immunotherapy for rectal cancer, they often investigate neoadjuvant immunotherapy approaches, sometimes even aiming to avoid surgery in highly responsive cases. Most advances still closely relate to developments in colon cancer, since both fall within the same disease spectrum. Progress in targeted immunotherapy continues to shape treatment strategies for various colorectal cancers.
Immunotherapy for Stage 3, Stage 4, and Metastatic Colon Cancer
The role of immunotherapy for bowel cancer depends on the stage, tumor-specific characteristics, and the extent of spread. In the early stages, it can be used as an addition to surgery to prevent the recurrence and target residual cancer cells. The best immunotherapy for metastatic colorectal cancer is determined by a multidisciplinary team and is usually integrated into a comprehensive treatment plan aimed to provide the patient with tumor control and a high quality of life.
Immunotherapy for Stage 3 Colon Cancer
During stage 3 of the disease, the cancer is locally advanced but has not yet spread to the distant organs. Immunotherapy for colon cancer stage 3 is increasingly being used as an adjuvant approach, especially for patients with MSI-H/dMMR tumors, to destroy any remaining cells after the surgery.
Immunotherapy for advanced bowel cancer is becoming a first-line option for selected high-risk cases, especially when standard chemotherapy is not well tolerated or when there is a strong immunogenic tumor profile. Treatments such as dendritic vaccines can assist not only in controlling the tumor locally but also in establishing long-term immunity to prevent recurrences.
The post-surgical timing window for adjuvant DC vaccination at stage 3 is clinically significant. The period immediately following resection — when the tumor's immunosuppressive microenvironment has been disrupted and antigen material from the surgical specimen is most current — offers the most favorable conditions for vaccine-induced immune activation. For international patients who require time to organize travel to Germany after surgery, that window narrows with each passing week.
Booking Health prioritizes the administrative timeline for post-surgical adjuvant cases, compressing document preparation, clinic communication, and travel logistics into the shortest possible interval so the vaccination occurs when the biology supports it most.
CHECK IF A BETTER SOLUTION EXISTS FOR YOUImmunotherapy for Stage 4 Colon Cancer
During stage 4, the disease spreads beyond its primary localization to distant organs and lymph nodes. Immunotherapy for colon cancer stage 4 plays an established role, with treatments like immune checkpoint inhibitors being integrated into the standards of care. Adoptive cell therapy, dendritic cell vaccination, and toll-like receptors as immunotherapy for stage 4 colon cancer are also showing great results in properly selected patients.
MSI/MMR status, tumor mutational burden, and other molecular testing help to determine the best stage 4 colon cancer immunotherapy, which will help extend survival and achieve tumor control.
Immunotherapy for Treating Metastatic Colorectal Cancer (Including Liver Spread)
For patients with metastatic disease, including common scenarios such as liver metastases, immunotherapy for metastatic colon cancer depends largely on tumor biology and treatment personalization. In patients with liver involvement, immunotherapy for colon cancer spread to the liver may be combined with surgery, ablation, or systemic therapies, depending on the extent of disease. This approach is determined by a team of specialists who evaluate the patient’s molecular profile, tumor burden, and overall condition.
As treatment strategies develop further, the use of immunotherapy for metastatic colorectal cancer continues to grow. Research explores combination therapies and identifies the most effective options for patients who do not initially respond to standard treatments.
For colorectal cancer with liver metastases specifically, the combination of TACE or ablation with immunotherapy is most effective when the two are sequenced within the biological window created by local tumor destruction — ablation-triggered antigen release enhances the subsequent immune response when vaccination or checkpoint inhibitor therapy follows within days, not weeks. For international patients, that window cannot be bridged across two separate trips: the ablation and the immunotherapy need to occur within the same Germany visit.
Booking Health structures combination programs around that clinical timeline from the outset, so the metastatic management strategy the multidisciplinary team recommends is the strategy the patient actually receives.
FIND THE RIGHT SPECIALIST FOR MY CASEHow is Colorectal Cancer Immunotherapy Carried Out?
Different approaches of immunotherapy for colon cancer treatment have their own timing and way of administration. Each method is individualized, and throughout therapy, patients are closely monitored to assess treatment response, detect potential immune-related side effects, and adjust the strategy as needed. This personalized approach guarantees that immunotherapy for colorectal cancer treatment can be both highly effective and safe for the patient.
The immune checkpoint inhibitors, for example, PD-1/PD-L1 and CTLA-4, are administered intravenously under medical supervision in either an outpatient or day hospital setting. The time intervals between doses are usually every 3-6 weeks, depending on the cancer treatment regimen. These agents are generally well tolerated and effective at stimulating the immune system, including T-cell activity.
The dendritic vaccines for the colon cancers are usually administered subcutaneously in a day hospital setting. In the case of dendritic cell vaccines, which create a target-specific immune response, a single injection will accomplish long-term anticancer immunity. This procedure is designed to instruct the immune cells to recognize and attack malignant cells, but leave the healthy tissues, which are not affected, intact. If desired, more injections can be given, depending upon the clinical needs of the patient.
The adoptive cell therapy necessitates an inpatient procedure because, usually, pre-treatment with high-dose chemotherapy is employed before the infusion of the modified CAR T-therapy, which is used for patients with advanced disease. The laboratory phase in the generation of CAR T-cells may take up to three weeks. Typically, two visits to the clinic are required. The first one is for the preparatory procedures, and the other is for the immunotherapy infusion. This individualized therapeutic approach directs the immune system against tumor proliferation, which often does not respond to conventional treatment modalities.
The toll-like receptor agonists and reformation of the gut microbiome are going to be used and analyzed in clinical research. These create a rapid immune response, stimulate the immune cells, and are on the brink of becoming an important area of colorectal cancer treatment.
Comparing the Effectiveness of Colon Cancer Treatment Methods
The approach to treating colon cancer varies based on the cancer's stage, tumor biology, and individual patient factors. There is no one-size-fits-all method, and the most successful strategy usually involves combining multiple approaches. Targeted immunotherapy for colon cancer has gained attention in recent years and complements treatments such as surgery, chemotherapy, and targeted therapy.
Surgery remains the main approach for localized colon cancer (stages I–III). The goal is a complete tumor removal with lymph node dissection. But often it is not used alone in colon cancer treatment. Immunotherapy can be added after resection to ensure that all cancer cells are destroyed and to lower the risk of recurrence.
Chemotherapy and targeted therapy are usually used after the surgery or in metastatic patients. It forms the core of treatment for most patients, especially those who do not have MSI-H/dMMR tumors.
When the molecular type of cancer is MSI-H or dMMR positive, this is one of the immunotherapy indications for advanced colorectal cancer. In these instances, it results in a lasting response and, for many patients, sustained disease control.
In modern oncology, combining different treatments frequently yields optimal results. Surgery, chemotherapy, targeted therapy, and immunotherapy can be administered either sequentially or together, depending on the disease stage and the patient's response. For instance, metastatic disease is typically addressed with a multimodal approach that includes systemic therapy, followed by surgery if tumors become resectable. Even with the best immunotherapy for metastatic colorectal cancer, combining it with other treatment modalities is often necessary.
Comparison of Key Colon Cancer Treatment Approaches
| Treatment Approach | Mechanism of Action | Response Rate: Stage 4 | Advantages | Limitations |
|---|---|---|---|---|
| Surgery | Physical removal of the primary tumor and lymph node | Low, <20% | Curative in early stages | Not feasible in widespread metastases; depends on resectability and patient condition |
| Chemotherapy | Destroys rapidly dividing cells non-specifically | less than 10% | Fast response, widely applicable | Systemic toxicity affects healthy cells |
| Immunotherapy | Activates the immune system to recognize and attack tumor cells | 60 - 80% | Durable responses, lower toxicity profile | Individualized manufacturing is available at specialized centers only |
| Targeted Therapy | Inhibits specific molecular pathways (e.g., EGFR, ALK) | 35 - 45% | High response rates, personalized approach | Resistance may develop, limited to specific mutations |
| Radiation Therapy | Uses ionizing radiation to destroy tumor cells locally | less than 15% | Effective local control, non-invasive | Limited systemic effect, risk of damage to surrounding tissues |
Benefits and Side Effects of Immunotherapy for Colon Cancer
In countries with a well-developed health system, immunotherapy for colon cancer patients is increasingly being instituted as a first line of treatment, while at first it was reserved for patients with advanced cancer, including those who have metastatic tumors or therapy-resistant tumors. The average survival rate of patients with metastatic colon malignancy is about 6 months after failure of chemotherapy and targeted therapy, since uncontrolled tumor growth has taken place, standard treatment has little or no effect in prolonging life. In these areas of limited medical resources, tumor resistance usually results in symptomatic and palliative care being the only means of treatment left to the physician.
The advent of immunotherapy has greatly changed this picture. For instance, adoptive cell therapy may now increase the average survival of patients with metastatic colon cancer from 14 to 28 months, since genetically modified T-cells and other immune cells can launch a potent immune attack against malignant cells in the host.
Following these successful efforts, immune checkpoint inhibitors and cancer vaccines have been introduced earlier in the course of the disease, usually after surgical excision of the primary tumor when it is possible. The earlier immunotherapy can be used, the more effective the treatment is, since the immune system is trained to attack remaining cancer cells before widespread metastases occur.
Clinical experience and research have shown that in patients who have received immunotherapy for advanced colorectal tumors, cytotoxic T-cells in the blood increase rapidly. This indicates that these immune cells attack both the primary tumor and metastatic sites, slowing disease progression and, in some cases, resulting in remission. This demonstrates the remarkable capabilities of modern oncology, harnessing the body’s defenses to control tumor growth and improve survival in patients with colorectal cancer.
Possible Side Effects of Immunotherapy
Immunology treatment for bowel cancer is usually considered a safe treatment due to its high personalization. But it can cause mild side effects in some cases. These can be:
- Skin reactions: rash and pruritus
- Increased fatigue and flu-like symptoms: fever, chills, and coughing
- Inflammation of the intestines, thyroid gland, lungs, or liver when using checkpoint inhibitors
All of these side effects are manageable and do not show a significant difference between colon and rectal cancer as part of the broader colorectal cancer group. The safety profile of immunotherapy depends mainly on the type of agent used and on how the patient’s immune system responds, rather than on where the tumor is located.
Colon Cancer Immunotherapy Treatment Centers in Germany
When receiving immunotherapy for colon cancer in Germany, you will be guaranteed high-quality, evidence-based oncology care, with your outcomes depending heavily on the precision diagnostics, advanced immunotherapy options, and coordinated, multidisciplinary care at the clinic you choose. Here are some helpful points to consider when choosing the right facility for you:
- Experienced specialist in immunotherapy for colorectal cancer
- Access to biomarker testing, such as microsatellite instability (MSI) and mismatch repair deficiency (dMMR)
- Access to the latest types of immunotherapy for rectal cancer and colon cancer, like immune checkpoint inhibitors, cancer vaccines (dendritic cell-based therapies), and adoptive cell therapies (ACT)
- Presence of a multidisciplinary tumor board
- Support for international patients
Clinics that provide immunotherapy for colon cancer treatment in Germany are internationally recognized and meet all those criteria that ensure high-quality care. They work within multidisciplinary teams, where expert tumor boards make treatment decisions together. Coupled with robust research programs and extensive international patient support, they ensure patients get safe, innovative, and well-coordinated care that keeps up with the latest advancements in oncology.
Cost of Colon Cancer Immunotherapy in Germany
The cost of immunotherapy for colon cancer treatment is different depending on the country, its healthcare system, and access to modern oncology services. The treatment cost of immunotherapy for colon cancer in Germany is usually lower than in other developed countries for several reasons. For example, the cost of dendritic cell therapy ranges from €20,000 to €38,000 in Germany, compared to €100,000–€150,000 in the USA. The high availability of modern technologies and reduced healthcare costs are key reasons for this. Meanwhile, in the USA, longer waiting times and high prices often result from limited access to medical care due to insurance restrictions. In other countries like Great Britain or Australia, modern immunotherapies are not widely available.
Below, you can see a comparison table of prices and availability of various immunotherapies across the globe.
Cost of Immunotherapy Treatment in Different Countries
| Country | Dendritic cell therapy price | CAR T-cell therapy price | Checkpoint inhibitors price |
|---|---|---|---|
| Germany | €20,000 - €38,000 | €450,000 - €550,000 | €20,000 - €40,000 for 1 cycle |
| USA | €100,000 - €150,000 | $500,000 - $750,000 | €50,000 - €60,000 for 1 cycle |
| Great Britain | Not available | Not available | €90,000 - €100,000 for 1 cycle |
| Australia | Not available | Not available | Not available |
Germany's DC therapy range — up to €130,000 less than the US equivalent, and unavailable in the UK and Australia at any price — makes the availability gap the primary argument for British and Australian patients, not the cost comparison. Patients coordinating through Booking Health pay the same bill as country citizens do, without the foreign patient fee.
A fully itemized budget is confirmed before any commitment is made, complication insurance of €200,000 is included as standard; unspent funds are returned after the program concludes.
Get full treatment coordination supportA Medical Journey for Colon Cancer Immunotherapy in Germany With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for already 12 years, Booking Health possesses solid expertise in creating complex management programs in each individual case. As a reputable company, Booking Health offers personalized treatment plans for colorectal cancer with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment.
We provide:
- Assessment and analysis of medical reports
- Development of the medical care program
- Selection of a suitable treatment location
- Preparation of medical documents and forwarding to a suitable clinic
- Preparatory consultations with clinicians for the development of medical care programs
- Expert advice during the hospital stay
- Follow-up care after the patient returns to their native country after completing the medical care program
- Taking care of formalities as part of the preparation for the medical care program
- Coordination and organization of the patient's stay in a foreign country
- Assistance with visas and tickets
- A personal coordinator and interpreter with 24/7 support
- Transparent budgeting with no hidden costs
Health is an invaluable aspect of our lives. Delegating management of something so fragile yet precious should be done only to experts with proven experience and a reputation. Booking Health is a trustworthy partner who assists you in pursuing stronger health and a better quality of life. Contact our medical consultant to learn more about the possibilities of personalized treatment with innovative methods for colorectal cancer with leading specialists in this field.
Booking Health holds ISO 9001 quality certification, reflecting well-established processes and strict quality control at every stage of the treatment journey — not just at the initial consultation, but throughout.

Immunotherapy Journey: Dendritic Cell Treatment with Booking Health













FAQ: Immunotherapy for Colon Cancer in Germany
Immunotherapy is a modern type of therapy that helps the body’s own immune system to recognize and destroy cancer cells. It is often based on tumors’ biological markers such as MSI-H or dMMR status.
It involves using medications to stimulate the patient's immune system to recognize and attack cancer cells. It targets specific proteins or receptors on the cancer cells, enhancing the body's natural defenses.
Benefits include a targeted treatment approach, fewer side effects compared to traditional therapies, and the potential for long-term remission by stimulating the immune system. It offers new hope for patients with advanced or resistant colon cancer.
Modern immunotherapy in Germany includes immune checkpoint inhibitors, dendritic cell vaccines, adoptive T-cell transfer, and experimental methods such as TLR agonists. These treatments help the immune system detect and attack tumor cells more effectively.
Dendritic cell therapy for colon cancer is showing promising results, especially in research. By stimulating the immune system to recognize tumor antigens, this therapy can slow disease progression, reduce relapse risk, and improve overall survival when combined with other treatments.
It can be used at any stage of the treatment as an adjuvant therapy after the surgery or in advanced cases to help control tumor growth and possibly achieve remission.
The cost of immunotherapy in Germany varies depending on the chosen method, the hospital, and the patient’s condition. Booking Health helps patients save up to 70% by arranging treatment directly with leading German clinics.
Success rate depends on the tumor's unique characteristics, but for personalized treatments like dendritic cell therapy, it can reach 85%. In MSI-H/dMMR patients, response rates can be significantly higher than chemotherapy alone.
Yes, it can be used at this stage for certain high-risk cases, especially if standard chemotherapy is difficult to tolerate or if the tumor has a strongly immunogenic profile.
Yes, Booking Health colon cancer support includes selecting the best clinic, negotiating costs, translating medical reports, and organizing the entire trip. Patients benefit from transparent pricing, professional guidance, and coordination throughout the whole treatment journey.
Stage 4 colon cancer immunotherapy can be effective in controlling tumor growth, especially when standard chemotherapy fails. It helps extend survival and improve quality of life by activating the immune system to attack cancer cells, even in advanced metastatic cases.
Yes, it can be used depending on the tumor’s biomarker status to slow progression, lower tumor burden, and maintain patients’ quality of life, especially if standard treatments are no longer an option.
Yes. In many cases, immunotherapy is used alone or combined with surgery, ablation, or systemic therapy, depending on whether metastases are resectable.
Common drugs include PD-1 and CTLA-4 inhibitors, dendritic cell vaccines, ALC, and toll-like receptors. They boost the immune system to recognize and destroy cancer cells more effectively.
It depends on the type of treatment and the patient's individual characteristics, ranging from a one-time administration of dendritic cell vaccines to a few months of intravenous outpatient injections for checkpoint inhibitors.
The side effects of immunotherapy are usually milder than those of chemotherapy. Patients may experience fatigue, appetite loss, diarrhea, or mild skin reactions. Most symptoms are temporary and manageable under medical supervision in German clinics.
You can begin by booking colon cancer treatment in Germany through Booking Health’s platform. Simply send your medical records, and their team will suggest the best options, provide cost estimates, and guide you through every step of the process.
Adding immunotherapy significantly increases the effectiveness of colon cancer treatment. At stage 3, the response rate to standard regimens increases from 50% to 80%, and at stage 4 from 30% to 50%. This approach improves survival and helps to achieve stable remission even with advanced disease.
At stage 4 colon cancer, standard treatment gives a positive response in 30–40% of cases, while adding immunotherapy increases the effectiveness to 50%. This means that even patients with metastases have a chance for stable improvement and prolongation of life.
Combining immunotherapy with standard colon cancer treatment activates the patient's natural immunity, enhances the effect of drugs, and reduces the risk of relapse. This approach increases the sensitivity of the tumor to therapy and promotes long-term remission without significant deterioration in well-being.
The cost of immunotherapy in the treatment of colon cancer depends on the type of drug, the stage of the disease, and the duration of the course. On average, the price is formed individually after diagnosis, but patients note that the results exceed the costs due to the long-term effect.
Yes. Immunotherapy for rectal vs colon cancer activates T-cells and other immune cells. Methods like vaccines and adoptive cell therapy for CRC target tumor cells, while protecting healthy tissue, improve outcomes even in advanced cases. Booking Health support of CRC immunotherapy in Germany ensures access to leading clinics, personalized protocols, and coordination for advanced treatment options.
Immunotherapy shows different patterns of effectiveness in rectal vs colon cancer, largely due to differences in tumor location and the local immune microenvironment. Rectal tumors often require both local and systemic immune activation, whereas colon tumors generally respond primarily to systemic therapy.
Yes. Immunotherapy combination for CRC with chemotherapy or radiation enhances immune response and tumor control, providing a synergistic effect that improves outcomes for both colon and rectal cancer patients.
Administration of immunotherapy for colorectal cancer is tailored to the tumor site. Studies evaluating the effectiveness of immunotherapy for rectal vs colon cancer show that colon tumors generally respond better to systemic therapy, whereas rectal tumors may require additional local immune activation for optimal results.
In Germany, colon cancer patients can access a full spectrum of immunotherapy options. Treatments are individualized and administered in specialized centers. Also, they are combined with standard oncology care to enhance immune response.
Choose treatment abroad and you will for sure get the best results!
Sources:
01. Sumin Wu, Yunping Zhang, Zi Lin, Min Wei. Global burden of colorectal cancer in 2022 and projections to 2050: incidence and mortality estimates from GLOBOCAN. BMC Cancer. 2025 Nov 14;25:1770. doi: 10.1186/s12885-025-15138-0. [DOI] [PMC free article]
02. Gholamreza Roshandel, Fatemeh Ghasemi-Kebria, Reza Malekzadeh. Colorectal Cancer: Epidemiology, Risk Factors, and Prevention. Cancers (Basel). 2024 Apr 17;16(8):1530. doi: 10.3390/cancers16081530. [DOI] [PMC free article]
03. C Richard Boland, Ajay Goel. Microsatellite Instability in Colorectal Cancer. Gastroenterology. 2010 Jun;138(6):2073–2087.e3. doi: 10.1053/j.gastro.2009.12.064. [DOI] [PMC free article]
04. Nitin Mishra, Jason Hall. Identification of Patients at Risk for Hereditary Colorectal Cancer. Clin Colon Rectal Surg. 2012 Jun;25(2):67–82. doi: 10.1055/s-0032-1313777. [DOI] [PMC free article]
05. Chiugo Okoye, My Tran, Elizabeth Soladoye et al. A Review of 10-Year Survivability of Immunotherapy in the Management of Colon Cancer. Cureus. 2023 Aug 9;15(8):e43189. doi: 10.7759/cureus.43189. [DOI] [PMC free article]
06. Norah A Alturki. Review of the Immune Checkpoint Inhibitors in the Context of Cancer Treatment. J Clin Med. 2023 Jun 27;12(13):4301. doi: 10.3390/jcm12134301. [DOI] [PMC free article]
07. Palaniyandi Muthukutty, Hyun Young Woo, So Young Yoo. Therapeutic Colorectal Cancer Vaccines: Emerging Modalities and Translational Opportunities. Vaccines (Basel). 2025 Jun 26;13(7):689. doi: 10.3390/vaccines13070689. [DOI] [PMC free article]
08. Mahmoud Singer, Jennifer Valerin, Zhuoli Zhang et al. Promising Cellular Immunotherapy for Colorectal Cancer Using Classical Dendritic Cells and Natural Killer T Cells. Cells. 2025 Jan 22;14(3):166. doi: 10.3390/cells14030166. [DOI] [PMC free article]
09. Liu C, Liu N, Zhang T and Tu Y (2025) Adoptive immune cell therapy for colorectal cancer. Front. Immunol. 16:1557906. doi: 10.3389/fimmu.2025.1557906. [DOI]
10. Tianhao Duan, Yang Du, Changsheng Xing, Helen Y Wang, Rong-Fu Wang. Toll-Like Receptor Signaling and Its Role in Cell-Mediated Immunity. Front Immunol. 2022 Mar 3;13:812774. doi: 10.3389/fimmu.2022.812774. [DOI] [PMC free article]
Read: