

When benign prostatic hyperplasia (BPH) forces a man to choose between medications that work incompletely and surgery that resolves one problem by creating others, the choice itself is part of the burden. Sexual dysfunction and incontinence are not acceptable trade-offs for men whose primary complaint is disrupted sleep and urinary frequency — which is why so many patients with BPH remain undertreated, tolerating signs and symptoms rather than accepting surgical consequences. Prostatic artery embolization was developed as a new player on the benign prostatic hyperplasia treatment market for exactly that gap. Minimally invasive, performed under local anesthesia, with patients returning to normal activity within 1–2 days — PAE reduces the prostate's blood supply, shrinks the gland, and delivers substantial prostate adenoma symptoms relief without the functional consequences that have historically made surgery a measure of last resort.
Benign Prostatic Hyperplasia: A Global Health Challenge
The scale of benign prostatic hyperplasia as a public health problem is not adequately captured by prevalence figures alone — though those figures are striking enough. Approximately 45% of men over 45 and around 80% of men over 70 are affected, with the global 65–69 age group carrying the highest burden and concerning upward trends emerging simultaneously in the 40–44 and 80+ groups. Middle-SDI regions bear the heaviest absolute load. The condition is expanding across age groups in both directions at once.
Behind those numbers is a daily reality that statistics compress into abstraction. Nocturia does not merely interrupt sleep — it prevents the sustained sleep architecture that cognitive function, mood, and physical recovery all depend on. Urinary obstruction and weak urinary stream impose a constant background awareness that shapes where a man can go, how long he can stay. Increased frequency turns travel, professional obligations, and uninterrupted social engagement into problems requiring active management rather than activities pursued without thought. The cumulative effect on quality of life and mental health is not incidental to the disease — it is the disease, experienced daily by men who are often told their condition is not serious enough to justify the risks of surgery and not responsive enough to justify continued medication. PAE exists because that answer is no longer the only one available.
Conventional BPH Management
The standard benign prostatic hyperplasia nonsurgical treatment sequence begins with medication — and for many patients, it also ends there. Not because the drugs resolved the problem of complications prevention and treatment. The surgical alternatives waiting on the other side of treatment failure have consequences that make symptom management feel like the lesser burden.
Alpha-blockers relax the smooth muscle of the bladder neck and prostate, easing urination without reducing the enlargement driving it. A different mechanism — 5-alpha reductase inhibitors block the hormonal changes that cause prostate growth, shrinking the gland gradually over months of uninterrupted use. Both deliver modest symptom relief. Both accumulate a side effect burden that erodes that relief over time: sexual dysfunction, dizziness, and hypotension are common enough to be expected rather than flagged as exceptional, and the prospect of indefinite medication with declining effectiveness is one that many men find as disruptive to daily life as the urinary symptoms it incompletely controls.
When medications are insufficient, surgery has a range of options — each representing a different trade-off between efficacy and risk rather than a clear clinical progression:
- Open prostatectomy, transurethral resection of the prostate, and transurethral incision — the surgical standard, with evidence bases built over decades.
- GreenLight laser treatment, transperineal laser ablation, and HoLEP — laser-based tissue reduction at varying degrees of invasiveness, each accesses the prostate with measurable risk.
- Aquablation — ultrasound-guided water jet tissue removal, newer in evidence but not categorically different in the functional risks it carries.
Bleeding, retrograde ejaculation, urinary incontinence, erectile dysfunction — these are not rare complications that patients are statistically unlikely to encounter. They occur at rates that make them predictable features of the surgical landscape rather than exceptional outcomes. General anesthesia, hospitalization, and recovery measured in weeks compound the decision's weight for men whose primary complaint was already disrupting their daily lives.
Minimally invasive benign prostatic hyperplasia alternative therapy — prostatic urethral lift, transurethral microwave therapy (TUMT), Rezum technique (Water Vapor Ablation) — reduces the procedural burden without closing the durability gap. Retreatment rates are higher. Results deteriorate faster. Most cannot be applied to prostates exceeding 80cc, excluding precisely the patients whose disease burden is most severe. Some produce delayed symptom improvement that extends the period of disruption rather than ending it.
What the full landscape of conventional options reveals is a structural problem rather than a technological one. Durable symptom relief requires approaches that carry serious functional risk. Functional preservation requires approaches that cannot sustain their results. Prostatic artery embolization was developed because that trade-off is not inevitable — it is a consequence of treating BPH through tissue removal or suppression rather than through the vascular mechanism that controls prostatic volume without disturbing the structures that surgical access consistently endangers.
Prostatic Artery Embolization: The Next Generation in BPH Treatment
PAE does not manage symptoms the way medication does, and it does not remove tissue the way surgery does. This new prostate adenoma treatment reduces blood flow to the enlarged prostate — causing the gland to shrink through ischemia while preserving the urinary and sexual function that surgical approaches consistently place at risk. The same clinical outcome. A fundamentally different biological route. That distinction is what makes PAE a paradigm shift rather than an incremental refinement of what already exists.
*Pisco JM et al Eur Radiol 2013;23(9):2561
How PAE Works
This new benign prostatic hyperplasia treatment begins with a puncture smaller than most patients expect — a single entry point in the femoral artery under local anesthesia, through which everything that follows is accomplished without a surgical incision, without general anesthesia, and without hospitalization beyond the day of treatment. A prostate interventional radiology specialist advances a microcatheter through the arterial system under digital subtraction angiography and cone-beam CT guidance, navigating to the prostatic arteries that supply blood to the enlarged tissue. Precision here is not a quality standard — it is what determines which tissue is treated and which is left entirely undisturbed. Small embolic particles, typically 100–500 μm in diameter, are injected to block those arteries, cutting off the blood supply that sustains the enlarged prostate and initiating the ischemic shrinkage that produces symptom relief over the weeks that follow. The nerves, sphincters, and surrounding structures that surgical approaches place consistently at risk are never approached — because a procedure that works through the arterial system has no reason to reach them.
PAE works through multiple synergistic mechanisms that make it particularly effective:
- Ischemic infarction leading to shrinkage of the enlarged prostate gland
- Relaxation of increased prostatic smooth muscle tone through α-adrenergic denervation (similar to the action of alpha-blockers)
- Nitric oxide-mediated relaxation of smooth muscle cells (analogous to phytotherapy)
- Interruption of the testosterone axis, providing androgen deprivation (similar to the progression-inhibition by 5α-reductase inhibitors)
- Ischemia-mediated apoptosis of prostate cells
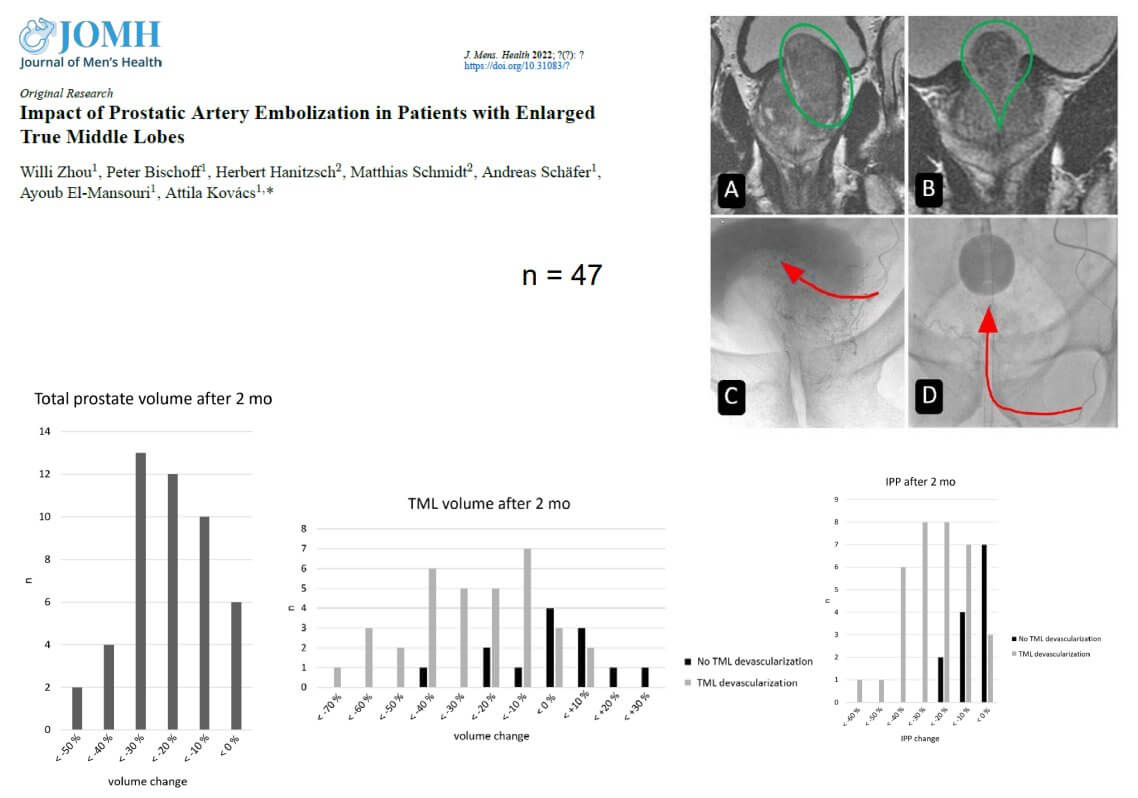
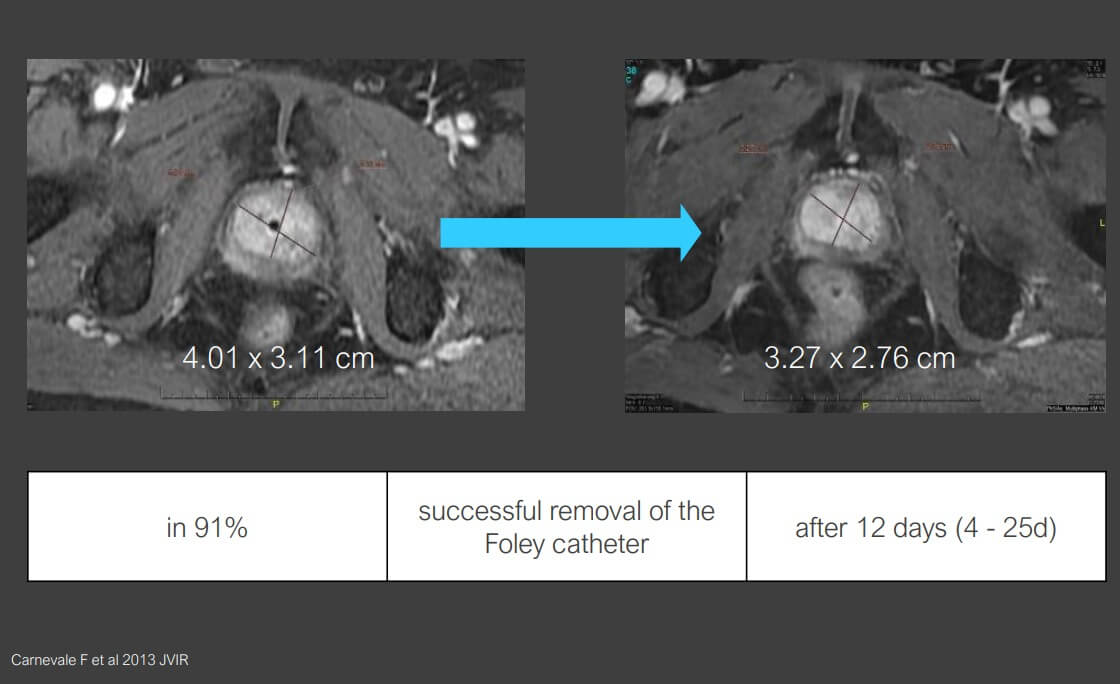
This multifaceted approach allows PAE to provide both immediate symptomatic relief and sustainable reduction in prostate volume over time. Importantly, PAE can effectively reduce specific prostatic structures that cause obstruction, including the intravesical prostatic protrusion (IPP) and true middle lobe (TML), which are often major contributors to bladder outlet obstruction and storage symptoms that particularly bother patients.
The navigation precision new treatments for benign prostatic hyperplasia require — a microcatheter guided through the femoral artery to the specific prostatic arteries feeding the enlarged tissue, confirmed by cone-beam CT at every critical step — is not a procedure that generalizes across interventional radiology centers. A specialist who performs PAE regularly develops an anatomical familiarity with the prostatic arterial variants that makes the bilateral approach technically achievable in cases where a less experienced operator might achieve only unilateral embolization. The outcome data above — 42.3% volume reduction in prostates greater than 80cc — applies to centers where bilateral PAE is the standard result, not the optimistic scenario.
Booking Health selects PAE centers based on annual procedure volume and documented bilateral success rates, because the difference between one-sided and two-sided embolization is the difference between partial and full clinical benefit.
CHECK IF A BETTER SOLUTION EXISTS FOR YOUIdeal Candidates for the Procedure
PAE is particularly the best treatment for benign prostatic hyperplasia in:
- Symptomatic patients with lower urinary tract symptoms (LUTS) that are moderate to severe as measured by the International Prostate Symptom Score (IPSS)
- Patients with impaired quality of life due to BPH symptoms
- Those who have not responded adequately to medical therapy for at least 6 months
- Patients who are not candidates for surgery or have refused a surgical intervention
- Men with prostatic volumes greater than 80cc that are too large for traditional TURP etc.
- Patients experiencing urinary retention medication needs
Research has identified several predictors of better clinical outcomes with PAE, including age less than 65 years, successful bilateral PAE (treating both sides of the prostate), lower baseline IPSS, and patients with urinary retention. Notably, patients with larger prostates (>80ml) often experience greater volume reduction (42.3% vs. 28.9%) and symptom improvement compared to those with smaller prostates.
*Data of Prof. Dr. med. Attila Kovács
The presence of a true middle lobe (TML) was previously considered a relative contraindication for PAE. Still, recent clinical studies have consistently demonstrated that PAE is effective as a procedure to alleviate problems caused by increased TML volume by approximately 32.1% when the TML is successfully embolized, with corresponding improvements in symptoms and urinary flow.
Each eligibility criterion above requires current urological data to confirm — prostate volume by MRI or TRUS, IPSS score from recent assessment, post-void residual urine measurement, etc.
A patient who was assessed six months ago during his latest treatment for benign prostate enlargement may have a different prostate volume and IPSS baseline.
Booking Health's pre-treatment case review identifies which of these measurements are current and which need updating before the PAE consultation is scheduled, so the interventional radiologist's first discussion with the patient is planning a new treatment for benign prostatic hyperplasia rather than a repeat diagnostic workup.
GET A SECOND OPINION FOR YOUR CASEKey Advantages over Traditional Methods
Interventional radiology and prostate artery embolization for benign prostatic hyperplasia offer several significant advantages over traditional BPH treatments:
- Minimally invasive procedure performed under local anesthesia
- No risk of TUR-related surgery side effects such as retrograde ejaculation, incontinence, or sexual dysfunction
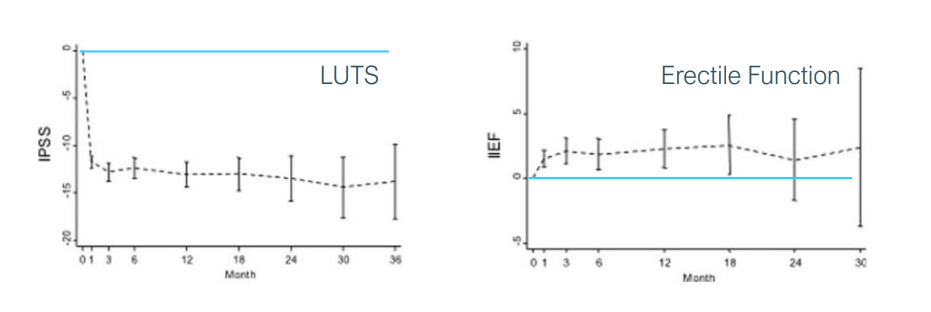
- Immediate effect, with LUTS improvement beginning after just 5-8 days
- The sustainable effect that continues to progress over the following 6 months
- Ability to reduce or eliminate medication use
- Particularly effective for storage symptoms (urgency and nocturia), which are often most bothersome to patients yet improve less with conventional surgery
- Exceptionally well-suited for patients with larger prostates (>80cc) who are not ideal candidates for TURP
- Very low retreatment rate of under 1% at 5 years
- Minimal side effects, with only about 8.5% of patients experiencing mild postembolization syndrome that can be effectively managed with non-steroidal anti-inflammatory drugs
As our research team has found, perhaps the most important advantage of PAE is its favorable side effect profile. The perioperative risks of bleeding and anesthesia complications, along with medium-term risks of urinary incontinence, effects on sexual function, and retrograde ejaculation associated with conventional treatments, are serious concerns for many patients. PAE's ability to avoid these complications leads to high patient satisfaction.
VIDEO
Prof. Atilla Kovács:
Why Prostate Artery Embolization is the Only Treatment That Improves Erectile Function
Interventional Radiology
BOOK CONSULTATION
Expected Results and Recovery Timeline: Conventional vs Novel
Treatment approaches for BPH vary significantly in terms of their results, recovery timelines, and overall impact on patients' quality of life. Based on our research and clinical experience, we've found that PAE offers a compelling balance of effectiveness and minimal disruption to patients' lives.
BPH Treatment Options: Comparative Outcomes & Side Effects
*Booking Health data
| Treatment | Volume Reduction | Symptom Improvement (IPSS) | Recovery Time | Side Effects | Retreatment Rate (5 years) |
|---|---|---|---|---|---|
| Medications | Minimal or none | Variable, often modest | None (ongoing treatment) | Variable, including sexual dysfunction, dizziness | N/A (ongoing treatment) |
| TURP | 30-80% | 10-15 point reduction | 2-4 weeks | Moderate (retrograde ejaculation in 65-75%, bleeding, longer recovery) | 10.3-11.6% |
| Aquablation | 30-35% | 10-12 point reduction | 1-2 weeks | Mild (catheterization, bleeding) | About 1% |
| Water vapor ablation | 15-30% | 10-12 point reduction | 3-5 days | Mild (temporary urinary symptoms) | 4.4-7.5% |
| PAE | Up to 42% for prostates >80cc | 10-15 point reduction | 1-2 days | Minimal ( temporary localized discomfort) | Under 1% |
PAE demonstrates particularly impressive results in several key areas:
- Prostate volume reduction: studies show an average reduction of 25.8% overall, with even greater reductions (42.3%) in patients with larger prostates (>80cc)
- Intravesical prostatic protrusion (IPP): successfully reduced by 29.3% on average when the procedure is technically successful, addressing a major contributor to bladder outlet obstruction
- Symptom improvement: significant reductions in IPSS scores (10-15 points), particularly for storage symptoms like urgency and nocturia that patients find most bothersome
- Quality of life: substantial improvements in quality of life scores
- Urinary flow: increase in maximum flow rate by 4.5-6 ml/s, with greater improvements in patients with larger prostates
- Residual urine: reduction of 60-80 ml in post-void residual urine volume
Recovery after PAE is remarkably rapid compared to conventional treatments. Most patients experience only mild discomfort for 24-48 hours, which can be effectively managed with over-the-counter pain medications. Many patients can return to normal activities within 1-2 days, compared to weeks of recovery required after surgical interventions.
Importantly, while LUTS improvement begins within 5-8 days after PAE, benefits continue to progress over 6 months as the prostate gradually shrinks, providing sustainable long-term relief.
The 1-2 day return to normal activities that distinguishes PAE from TURP's 2-4 week recovery is not only a quality-of-life advantage — for international patients it is a logistical one.
A man who travels from Australia, the US, or the Middle East for PAE can realistically complete the procedure and the immediate post-procedure observation within a single short visit to Germany, then return home to continue the 6-month improvement trajectory without a prolonged in-country stay.
Booking Health structures the visit around that recovery profile: pre-procedure documentation and imaging are completed before arrival, the procedure and 24-48 hour observation period are organized within a single coordinated stay, and post-treatment communication between the patient's home urologist and the German interventional radiology team is maintained throughout the 6-month follow-up window.
Accessing World-Class PAE Procedure with Booking Health
PAE is a novel nonsurgical procedure used to treat benign prostatic hyperplasia, not a procedure that any interventional radiology department can perform to the standard that makes it a genuine alternative to surgery. Extensive experience in embolization technique, precise knowledge of prostatic vascular anatomy, and cone-beam CT imaging infrastructure are not supplementary credentials — they are what separates a procedure performed safely from one performed adequately. That level of specialization exists in relatively few centers worldwide, which means the gap most patients face is not between deciding to pursue PAE and finding a facility that offers it. It is between finding a facility that offers it and finding one that has performed it enough times to do it well.
Booking Health identifies that distinction and acts on it. For patients seeking PAE as a meaningful alternative to medication or surgery, the support covers every stage of the process:
- Case assessment by specialists who evaluate prostatic anatomy, symptom profile, and clinical priorities before any facility recommendation is made — because the right center for one patient's vascular anatomy is not automatically right for another's.
- Connection to internationally recognized facilities whose interventional radiologists have documented procedural volume in PAE specifically, without the foreign patient charges that inflate treatment costs for patients traveling abroad.
- Complete coordination of medical documentation, appointments, and insurance coverage as a unified process — not a checklist the patient manages between other demands.
- Travel logistics including transportation and accommodation, interpreter services.
- Post-treatment care management that continues after the patient returns home. This includes supportive therapy procurement, specialist communication, and follow-up continuity that treats recovery as part of the program rather than as what happens after it ends.
A prostate adenoma diagnosis presents treatment options that look similar on paper and differ substantially in execution — which is why matching patient to specialist matters as much as matching patient to procedure. Booking Health's case review ensures both alignments are made before the patient travels, not after they arrive. The goal is not access to PAE in the abstract. It is access to the PAE result that changes how a patient lives — and that goal begins with choosing the right hands to perform it.
Booking Health holds ISO 9001 quality certification, reflecting well-established processes and strict quality control at every stage of the treatment journey — not just at the initial consultation, but throughout.

Every Patient Has a Story: Booking Health Treatment Journeys that Inspire










Frequently Asked Questions of Our Patients
Benign prostatic hyperplasia is a non-cancerous enlargement of the prostate gland — not a disease that develops suddenly, but a gradual biological process that affects approximately 45% of men over 45 and around 80% of men over 70. As the gland grows, it compresses the urethra and disrupts urinary function, causing symptoms of benign prostatic hyperplasia: frequent urination, difficulty initiating flow, incomplete bladder emptying, and the nocturia that fragments sleep night after night.
The right treatment is determined by prostate size, symptom severity, comorbidities, and what the patient is prepared to accept in terms of recovery and functional risk. Medication manages symptoms without addressing the enlargement itself. When pharmacological options prove insufficient, non-pharmacological treatment for benign prostatic hyperplasia — particularly prostatic artery embolization — offer substantial and durable symptom relief with a side effect profile that conventional surgery cannot match.
Combination therapies and PDE5 inhibitors have expanded the pharmacological benign prostate enlargement treatment, but the improvement they deliver remains modest and the side effects that accompany long-term use remain significant. For patients whose symptoms exceed what medication can adequately control, interventional approaches that address the anatomical cause of obstruction rather than its downstream effects represent a more decisive clinical solution.
No, benign prostatic hyperplasia does not increase prostate cancer risk. Despite both becoming more common with age, they are distinct conditions with different risk factors and cellular mechanisms.
Prostate size is the variable that most immediately constrains the options available — many minimally invasive procedures are unsuitable for glands exceeding 80cc. Beyond that, benign prostatic hyperplasia symptoms severity, overall health status, and the patient's specific priorities around sexual function, recovery duration, and side effect tolerance determine which approach fits. The same symptom burden in two different patients may call for entirely different interventions depending on what each is willing to trade for relief.
Where conventional surgery options trade functional risk for symptom control, newer approaches — and PAE in particular — deliver comparable symptom improvement without the rates of retrograde ejaculation, erectile dysfunction, and incontinence that surgical tissue removal produces. The clinical outcome is similar. What the patient keeps afterward is not.
Prostatic artery embolization, Aquablation, Rezum water vapor therapy, UroLift, and laser therapies each reach the prostate through a different mechanism — vascular, waterjet, thermal, mechanical, and ablative. No single approach is universally superior; each is most effective for a specific patient profile defined by prostate anatomy, symptom pattern, and clinical priorities. The most advanced treatment available is the one matched correctly to the patient receiving it.
PAE reduces prostate volume by blocking the arteries supplying blood to the enlarged gland — no surgical incision, no general anesthesia, no hospitalization beyond the day of treatment. Men with severe symptoms that have not responded to medication, prostates larger than 80cc that exclude them from most other minimally invasive options, and those for whom sexual function preservation is a clinical priority are the patients for whom PAE offers the most compelling clinical case.
A robotically-controlled waterjet guided by real-time ultrasound removes prostate tissue with a consistency that manual surgical technique cannot replicate across operators and anatomical variations. Thermal injury risk is lower than with laser approaches, operator variability is reduced by the robotic guidance system, and the technique remains effective across prostate sizes that limit other procedures — making it particularly valuable for patients with large or anatomically complex glands.
Is laser therapy still considered a viable option for BPH, and how does it compare to newer treatments?
Laser therapy remains a clinically meaningful option — particularly for patients whose anticoagulation status or overall health makes the bleeding risk of conventional TURP unacceptable. It offers reduced blood loss and shorter catheterization compared to traditional resection. For patients whose priorities center on avoiding general anesthesia or protecting sexual function, PAE addresses those concerns more directly — which is why the choice between approaches is always patient-specific rather than a simple ranking of old against new.
PAE produces temporary mild pelvic discomfort or low-grade fever in some patients in the days following the procedure — a physiological response to embolization that resolves without intervention. Aquablation requires a period of catheterization during recovery. Rezum can temporarily worsen urinary symptoms before treated tissue resolves and improvement emerges. What none of these approaches produces at meaningful rates is the retrograde ejaculation, erectile dysfunction, and incontinence that remain predictable features of a common surgical procedure — and that distinction is precisely what makes them worth pursuing.
Choose treatment abroad and you will for sure get the best results!
Sources:
01. Nature
02. National Institutes of Health (NIH)
03. Yale Medicine
Read:
01. HoLEP – painfree cure of benign prostatic hyperplasia (BPH)
02. Transurethral resection in treatment of benign prostatic hyperplasia
03. Aquablation in Germany: a promising prostate pathologies treatment





