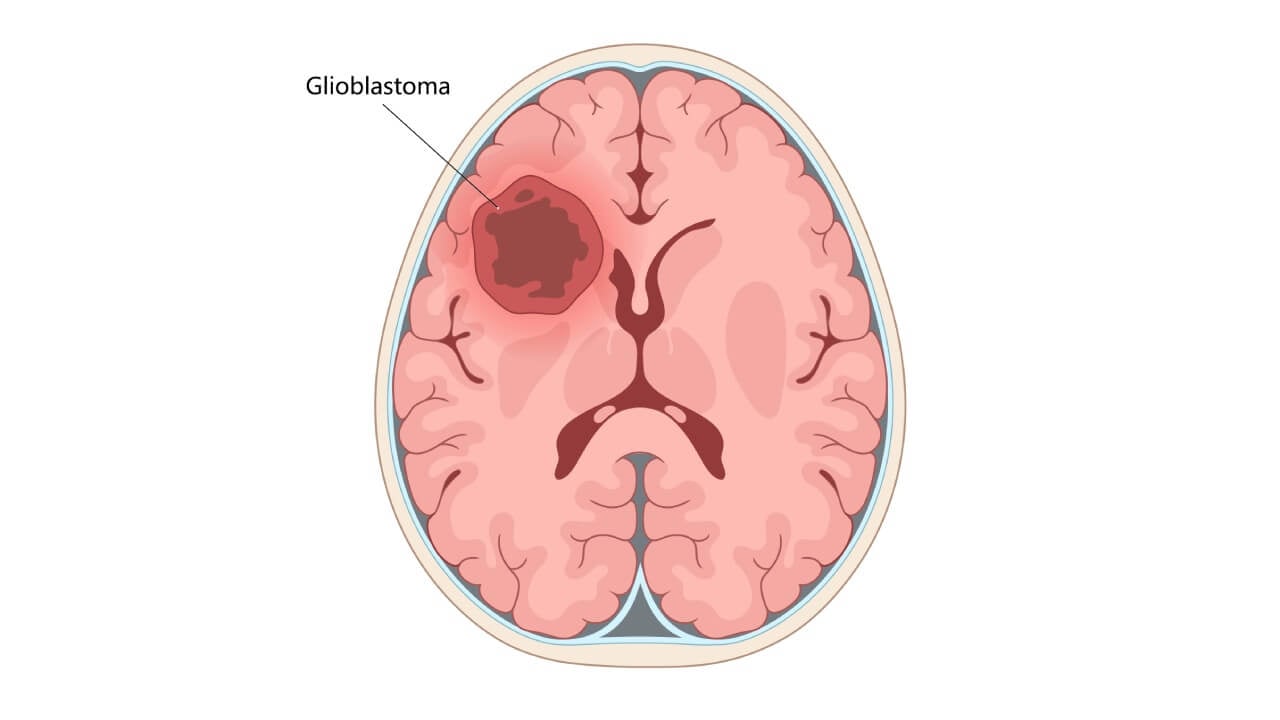
Glioblastoma (GBM or glioblastoma multiforme) is considered one of the most aggressive forms of brain cancer. Newly diagnosed GBM patients, according to global statistics, number approximately 3-5 per 100,000 population annually [1]. Specifically, in Germany, data from the 2022 national cancer registries show that about 3,130 women and 4,180 men were diagnosed with malignant central nervous system tumors that year. Many of those tumors represented high-grade gliomas (HGG), including GBM. To be more exact, the incidence of glioblastoma in this country ranges from 1.6 to 4.3 cases per 100,000, depending on age, sex, and region.
When looking at these data, many might notice that GBM has a relatively low incidence. However, brain tumors present a significant burden, as they are associated with a very poor prognosis. Data demonstrate that median overall survival under current standard-of-care (surgery + radiation + chemotherapy) remains in the range of 10-15 months; 5-year survival rates linger below 5-10 %. To support these data with evidence, there was a large retrospective study conducted in Germany. It involved over 40,000 adult GBM cases (1999-2014), which showed a median OS of 10.0 months; modest improvements were noted in 2-year survival rates over time (from 16.6 % → 19.3 %) [2].
In view of the information provided above, we want to suggest immuno-oncology (IO) as a promising approach for GBM patients. It works by utilizing the patient's immune system to selectively attack brain cancer cells while sparing normal cells. As an innovative treatment strategy, IO aims to train or reprogram immune cells to distinguish malignant from healthy tissue. Conventional treatments alone can rarely prevent relapse in patients with primary brain tumors. IO can potentially improve patient outcomes and survival. So, it is no wonder that it may seem especially appealing to those affected by GBM.
Why Immunotherapy Matters in Glioblastoma
The development of such a direction as immunotherapy for glioblastoma multiforme is due to the critical medical need for innovation. Standard treatment protocols, which have not changed for decades, have practically exhausted their resources. Glioblastoma remains one of the most challenging targets in oncology: even with the full multimodal approach, the median overall survival is only 12-16 months, which emphasizes the urgent need for innovative GBM immunotherapy [3].
The limited effectiveness of existing protocols is due to both the intrinsic mechanisms of tumor resistance and the complexity of its biological structure. That is why the most promising way to overcome this disease is considered to be brain tumor immunotherapy. Glioblastoma multiforme immunotherapy aimed at activating the patient`s own immune system to recognize and destroy cancer cells.
This direction has already demonstrated significant success in the treatment of other types of solid tumors (for example, melanoma or lung cancer), but the connection between immunotherapy and glioblastoma creates a unique set of obstacles due to the brain`s complex biology.
The use of immunotherapy for glioblastoma faces three critical barriers:
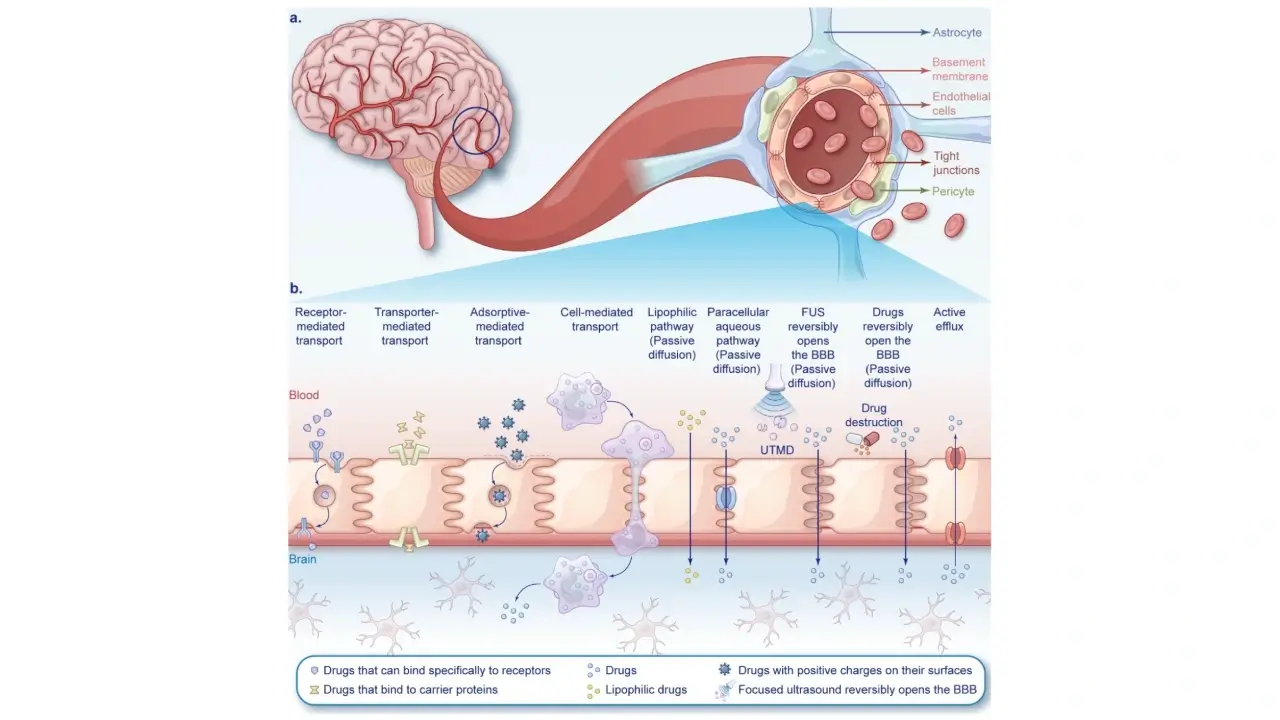
- Blood-Brain Barrier (BBB): A physiological filter that limits the penetration of therapeutic agents and immune cells from the bloodstream directly to the tumor.
- Immunosuppressive microenvironment: Glioblastoma secretes specific cytokines and involves regulatory cells that literally "turn off" local immunity, creating a significant barrier for the immune therapy of glioblastoma.
- Genetic and antigenic heterogeneity: High mutational variability allows the tumor to avoid immune recognition due to loss of target antigens, posing a challenge for glioblastoma immunotherapy [3]
- Surgical limitations: Typically, surgeons aim for "maximal safe resection". However, the infiltrative margin means that microscopic tumor cells always remain.
Despite the complexity of tumor biology, modern innovative immunotherapy is rapidly developing, offering solutions that are able to effectively overcome the above-mentioned obstacles. Brain cancer immunotherapy in Germany is based on the use of advanced technologies that systematically solve the problem of glioblastoma resistance.
Types of Immunotherapy for Glioblastoma
Types of immunotherapy for glioblastoma include strategies aimed at activating or enhancing the patient's immune system to identify and destroy tumor cells. This approach is traditionally divided into three main forms:
- Active immunotherapy: Stimulates the body's own protective resources (for example, vaccines).
- Passive immunotherapy: Uses external agents, like monoclonal antibodies, to enhance the response.
- Adaptive immunotherapy: It involves the modification of the patient's immune cells outside the body (ex vivo) with their subsequent return [4]
As we mentioned above, conducting effective immunotherapy of malignant brain tumors is complicated by the presence of a blood-brain barrier (BBB), high antigenic heterogeneity, and an immunosuppressive microenvironment that blocks the activity of T-lymphocytes.
Monoclonal Antibodies and Immune Checkpoint Inhibitors for Glioblastoma
Immune checkpoint inhibitors (ICIs) focus on blocking the signaling pathways that the tumor uses to self-mask and "turn off" immunity. These drugs are the most clinically mature immunotherapies evaluated for GBM in Germany and worldwide. Monoclonal antibodies (mAbs) and immune checkpoint inhibitors (ICIs) are the most clinically mature immunotherapies evaluated for GBM in Germany and worldwide. To explain broadly, mAbs either (a) bind tumor antigens or growth-factor pathways on GBM cells (e.g., EGFR, VEGF) to disrupt signaling, or (b) modulate T-cell activity by blocking inhibitory receptors (PD-1/PD-L1, CTLA-4). ICIs are mAbs by design. However, their goal is different: to release brakes on T-cells rather than to directly bind a tumor receptor.
Mechanism: Receptor blockade (such as PD-1, PD-L1, and CTLA-4) allows the "removal of brakes" on T-cells, restoring their ability to attack cancer [5].
Prospects: Neoadjuvant administration (before surgery) and combination of ICI with radiotherapy, laser thermal therapy (LITT), or new checkpoint molecules (LAG-3, TIM-3) are studied. This makes immunotherapy treatment for GBM more comprehensive and adaptable [5].
Limitations and why results are variable:
- Not all GBM cells overexpress the same receptor (e.g., EGFR/EGFRvIII may be subclonal), so direct anti-EGFR strategies can miss large fractions of the tumor.
- GBM features sparse effector T-cell infiltration, multiple redundant suppressive pathways, and steroid use. These are factors that blunt ICI efficacy.
- Certain agents often improve imaging and symptoms (PFS, edema control) without extending survival. This can be useful clinically, but frustrating for overall survival endpoints.
PD-L1 expression status and MGMT promoter methylation are the two molecular data points most directly linked to ICI and chemotherapy response in GBM — and both are frequently absent from the records of patients who were diagnosed and initially treated outside Germany's academic hospital network. A patient whose ICI eligibility is being assessed without confirmed PD-L1 characterization is being evaluated against statistical averages rather than their own tumor's biology.
Booking Health's pre-treatment case review identifies which molecular profiling has been performed and arranges any missing testing in Germany before the immunotherapy protocol is finalized.
CHECK IF A BETTER SOLUTION EXISTS FOR YOU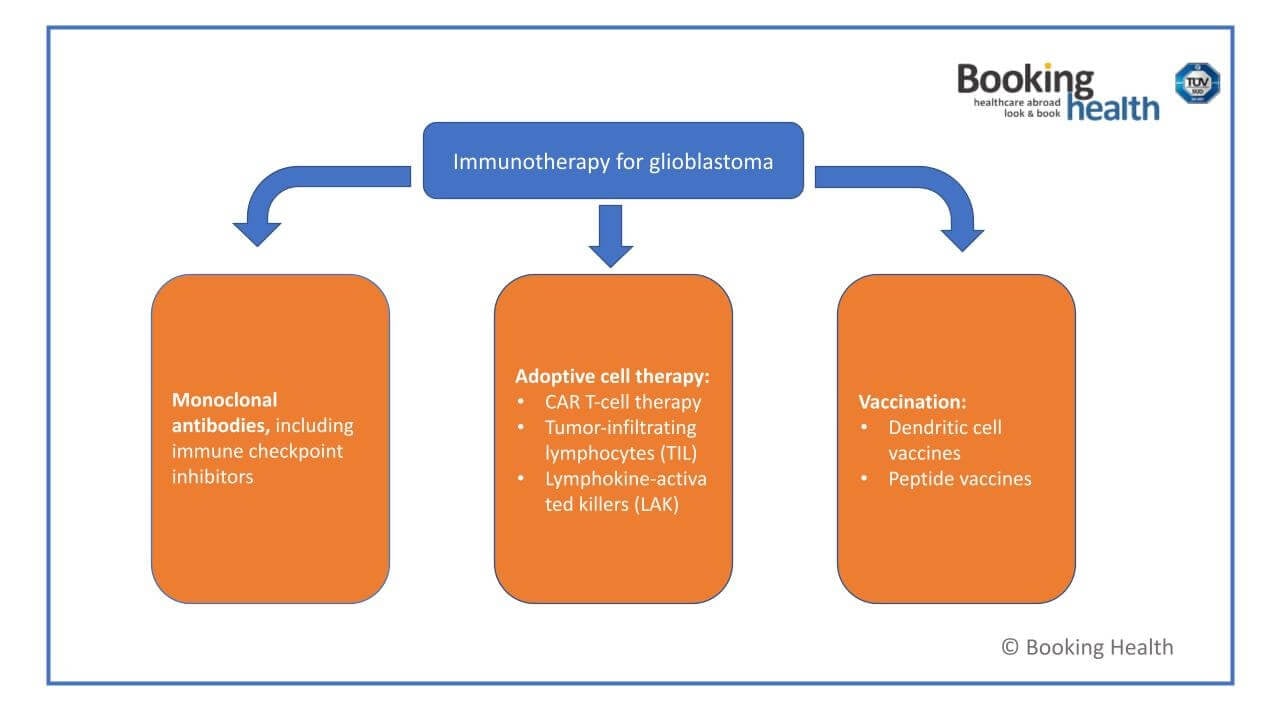
CAR T-Cell Therapy and Adoptive Cell Therapy for Glioblastoma
Adoptive cell therapy (ACT), in particular the use of CAR-T cells, is based on genetic modification of the patient's lymphocytes. This allows them to recognize specific tumor antigens without the involvement of the major histocompatibility complex.
Targets and innovations: EGFRvIII, IL13Rα2, HER2, and GD2 antigens are being studied. To combat tumor heterogeneity, "armored" CAR-T cells are created, which are able to secrete stimulating cytokines directly in the affected area [4].
Delivery: Local-regional administration (directly into the tumor or ventricles of the brain) shows higher efficiency, as it allows bypassing the BBB. This is an important step in the development of immunotherapy on brain tumors.
Related ACT approaches in GBM include:
- TIL therapy (tumor-infiltrating lymphocytes): harvest naturally tumor-reactive T cells from resected GBM tissue, expand ex vivo, then reinfuse (systemically or locoregionally). Modern protocols select CD137⁺ tumor-reactive TILs and show feasibility with evolving response signals.
- LAK cells (lymphokine-activated killers): earlier-generation ACT using peripheral lymphocytes expanded with IL-2.
There are certain limitations associated with utilizing this approach. First, commercial CAR-T list prices reimbursed in Germany range ~€282,000-€420,000 per dose (hematologic indications). Total episode costs commonly reach €400,000-€500,000 when manufacturing, hospitalization, CRS/ICANS management, and follow-up are included. Solid-tumor programs can be even higher. Hence, patient-specific GBM programs often cite €450,000-€550,000.
Second, antigen heterogeneity, limited T-cells within the tumor, and major immunosuppression produce transient responses in many studies. Consistent overall-survival gains over standard care have not yet been proven. In addition, cytokine release syndrome (CRS) and neurotoxicity (ICANS) require professional monitoring – this is another reason why care is centralized.
Dendritic Cell Vaccines and Peptide Vaccines for Glioblastoma
Vaccines, as a kind of immunotherapy for glioblastoma, aim to "train" the immune system to recognize tumor proteins and form long-term immune memory.
Dendritic cells and their role in adaptive immunity were discovered by Ralph M. Steinman, a Canadian immunologist, who was awarded the 2011 Nobel Prize in Physiology or Medicine for this work [7].
Dendritic cell vaccines (DCs): The patient's cells are "loaded" with tumor material ex vivo. Studies have shown a significant improvement in overall survival when such vaccines are used [8].
Peptide vaccines and personalization: Using short fragments of proteins helps activate cytotoxic T-cells. The main vector today is the creation of personalized vaccines based on the unique mutational profile (neoantigens) of a specific patient [1].
For a better understanding of the differences between the two most promising vaccine strategies, consider the comparative characterization of peptide and dendritic cell vaccines in the table below:
Peptide Vaccines vs. Dendritic Cell Vaccines in GBM
| Feature | Peptide Vaccines (e.g., IDH1 R132H, EGFRvIII) | Dendritic Cell Vaccines (e.g., tumor-lysate-loaded DCVax-L) |
|---|---|---|
| Antigen source | Defined synthetic epitope(s) | Patient-specific tumor lysate/peptides/mRNA |
| Personalization | Semi-personalized (mutation- or target-restricted) | Highly personalized (broad antigen repertoire) |
| Rationale | Focused immunity against a single dominant target | Poly-antigen response to mitigate antigen escape |
| Administration | Repeated subcutaneous/intradermal injections | Intradermal (often outpatient) |
| Costs (Germany) | Variable | €20,000-€38,000 baseline program costs (can rise with add-ons) |
Daria's case — described later in this article — illustrates the timing variable that determines how much of the DC vaccine's benefit is realizable. She traveled within 3-4 weeks post-surgery, which placed the vaccination inside the window when the tumor's immunosuppressive microenvironment is most disrupted and residual antigen from surgical resection is most current. A patient who delays that window by several months — while navigating clinic selection, document preparation, and visa processing independently — arrives for vaccination at a biologically different moment.
Booking Health compresses the administrative timeline by running documentation, clinic communication, and travel logistics simultaneously, because in GBM the question of when the patient receives the vaccine is as clinically significant as which vaccine they receive.
Get full treatment coordination supportOncolytic Viruses and Emerging Immune-Based Strategies for Glioblastoma
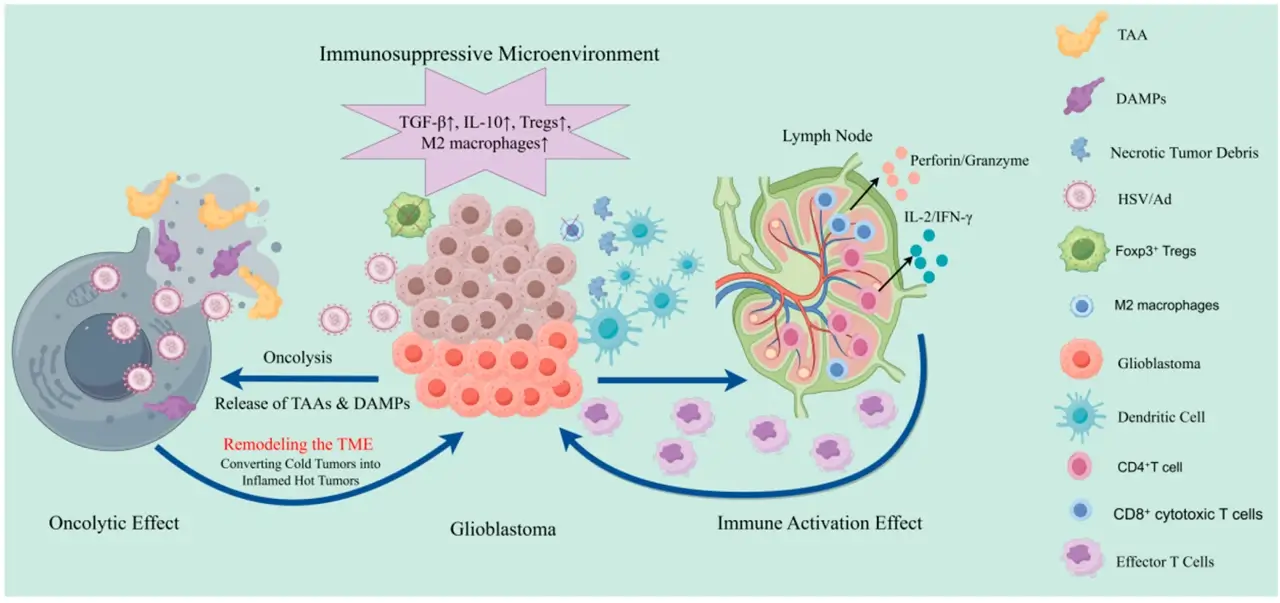
Oncolytic virotherapy (OVs) is also an immunotherapy for the treatment of glioblastoma, which uses modified viruses (herpes, adenoviruses, polioviruses) that selectively destroy cancer cells. In the management of GBM and other brain tumors, this action – direct lysis plus immune stimulation – makes OVs a strategy worth considering to be able to fight against the disease.
Double effect: Viruses cause direct destruction (lysis) of cells and, at the same time, release antigens that turn an "immunologically cold" tumor into a "hot" one, stimulating an immune response.
New Horizons: Promising strategies include the usage of genetically modified myeloid cells for interferon delivery, the application of STING agonists, and the integration of immunotherapy with electric field therapy (TTFields) [6].
However, we would like to add that oncolytic viruses are rarely used in isolation, as they are most effective when used in combination with immunotherapy. For example:
- OV + ICIs: OVs may upregulate PD-L1 or other checkpoints, making a tumor more sensitive to ICIs.
- OV + CAR-T/TIL/ACT: OVs can prepare the microenvironment, breaking down barriers to T-cell trafficking.
- OV + vaccine/DC therapy: Viral lysis provides fresh antigen substrate; vaccines supply defined epitopes.
- OV + standard therapy (chemo/radiation): Radiation or certain chemotherapeutics may increase viral replication or antigen release, enhancing OV efficacy.
Similar to other methods discussed in this article, there are certain considerations and challenges associated with the implementation of OVs.
First, intratumoral injection is often necessary; systemic routes risk neutralization or off-target effects. Second, neurotoxicity, inflammation, viral recombination, and viral shedding must be managed, especially in the CNS.
Moreover, preexisting immunity (e.g., to HSV, adenovirus) may blunt OV replication and effectiveness. Lastly, single-virus targeting may miss antigen-negative clones, demanding polyvalent or engineered approaches.
How Immunotherapy Is Used to Treat Glioblastoma
The usage of immunotherapy in glioblastoma has moved from the concept of simple "complementary therapy" to complex strategies aimed at overcoming the biological protection of the tumor. The main goal of immunotherapy for brain tumor is not only to destroy cancer cells, but also to fundamentally change the tumor microenvironment, which usually suppresses any immune activity.
The modern logic of using immunotherapy treatment for glioblastoma in Germany and other leading medical centers is based on the following principles:
- Purposeful engineering and overcoming barriers: Locoregional delivery of drugs is used, which allows immunotherapy directed to brain tumors to bypass the blood-brain barrier and act as targeted as possible.
- Creating immune memory: Unlike chemotherapy, immunotherapy teaches the body to recognize infiltrative glioblastoma cells, which is critical to preventing relapses.
The implementation process of GBM immunotherapy in Germany is organized as a clear cycle combining the biological preparation of the organism and high-tech work with cells.
It all starts with the first day dedicated to detailed planning. During the 30-minute consultation, the doctor collects an anamnesis, formalizes consent, and discusses with the patient a comprehensive strategy, including diet and complementary support methods that enhance the effect of immunotherapy for brain tumors.
The second day visit (lasting about 90 minutes) focuses on the collection of biomaterials. In the morning, 150-200 ml of blood is taken from the patient, from which cells will later be isolated for laboratory modification. This is immediately followed by a vitamin infusion (vitamins C and B) and an intramuscular injection of vitamin D (50,000 IU). This is necessary for the immediate activation of natural killers (NK cells) – the first line of defense of immunity.
The culmination of treatment falls on the ninth day. The patient is injected with prepared dendritic cells. Intradermal injection (into the skin) ensures their best migration to lymph nodes for "learning" T-lymphocytes. The procedure is followed by repeated infusions of vitamins and an injection of vitamin D. At the end of the visit, the patient is recommended a maintenance regimen of vitamin D (40,000 IU per week), which allows to consolidate the success of glioblastoma immunotherapy in Germany and ensures a long-term immune response against the tumor.
Comparing the Effectiveness of Glioblastoma Treatment Methods
A comparison of the effectiveness of modern glioblastoma treatment methods demonstrates a gradual transition from aggressive mechanical influence to subtle intellectual manipulation of the immune system. For decades, the basis of therapy remained a standard protocol combining the surgical resection, radiation therapy, and chemotherapy. While this approach allows for rapid reduction in tumor mass and primary control, it almost always faces the limit of its capabilities due to microscopic tumor debris that inevitably leads to recurrence.
That is why modern medicine views brain tumor immunotherapy treatment options as a useful addition to the basic scheme. They offer dynamic protection, allowing the immune system to adapt to the evolving nature of the tumor. For example, checkpoint inhibitors are aimed at removing molecular masking from a tumor. Although their effectiveness as an independent intervention has been limited, the usage of these drugs before surgery or in combination with radiotherapy demonstrates the ability to significantly enhance the local immune response.
Modern medicine offers increasingly personalized brain tumor treatment options. Immunotherapy, such as CAR-T cell therapy and adoptive cell therapy (ACT), takes treatment accuracy to a whole new level. As we know, these methods involve genetically reprogramming the patient's own lymphocytes to attack specific glioblastoma proteins. Although this method is extremely powerful, it requires continuous improvement to overcome the antigenic variability of the tumor. In this aspect, dendritic cell vaccines appear as one of the most stable strategies: they not only attack the tumor, but "train" the immune system to create long-term memory, which is confirmed by data on a significant increase in overall survival in the long term.
The synergy of methods is considered the most promising direction today. GBM immunotherapy clinics are increasingly adopting these combined protocols to offer patients a more comprehensive and personalized approach to treatment. Combining immunotherapy with radiation therapy allows the use of cancer cell death to stimulate immunity further, and co-administration with electric field therapy (TTFields) creates double pressure on the tumor, disrupting its separation at the physical and biological levels at the same time. Comparing methods thus indicates that the future treatment of glioblastoma is not to choose a single "best" remedy, but to build an individual treatment ecosystem in which each method enhances the action of the others.
Below is a comparative characterization of the main therapeutic lines, which allows you to assess the potential of each method in the context of prolonging the patient's life and preventing relapses.
Comparative Analysis of Glioblastoma Treatment Strategies
| Type of treatment | Main mechanism of action | Role in therapy | Advantages | Limitations |
|---|---|---|---|---|
| Standard protocol (surgery + radiation therapy + systemic therapy) | Physical removal and cytotoxic destruction of cells | Basic therapy (first line) | Rapid reduction of tumor mass, brain decompression | High probability of recurrence, toxicity to the body |
| Checkpoint inhibitors | Blocking of molecules that "sprinkle" immunity | Adjuvant or neoadjuvant therapy | Helps the immune system to "see" the tumor | Low effectiveness as monotherapy in glioblastoma |
| Dendritic cell vaccines (DC Vaccines) | Teaching immune cells to recognize tumor antigens | Personalized immunotherapy | Creating long-term immune memory, low toxicity | Complex and long manufacturing process |
| CAR-T/Adoptive therapy (ACT) | Using genetically modified T-lymphocytes | High-precision target attack | Aptitude to destroy specific mutant cells | The tumor can "run away" from the attack, changing the protein composition |
| TTFields (Electric fields) | Disruption of the process of cell division with the help of physical fields | Addition to maintenance therapy | Non-invasiveness, absence of systemic side effects | Need to constantly wear the device (up to 18 hours a day) |
| Combined protocols (Synergy) | Combination of immunotherapy with radiation or TTFields | Strategy of choice to overcome resistance | Highest potential to increase overall survival | Higher cost and difficulty of coordinating treatment |
Benefits and Limitations of Immunotherapy for Glioblastoma
Overall, immunotherapy (IT) has become an important investigational and clinical option for brain cancer, particularly glioblastoma (GBM). No single modality has yet become a universally adopted standard. However, the research evidence from programs in Germany highlights that it is necessary to consider both the strengths and the challenges of this approach.
Benefits of Immunotherapy in GBM
First, as we discussed, DC vaccine studies suggest that IT can extend the interval before tumor recurrence. In particular, this can be observed in patients who begin therapy shortly after maximal surgical resection and standard chemoradiation.
Second, IT (e.g., dendritic cell vaccines or CAR-T) is customized to the individual's tumor profile. By targeting patient-specific GBM cells or neoantigens (e.g., IDH1 mutations, EGFRvIII), these therapies account for GBM's heterogeneity better than "one-size-fits-all" chemotherapy.
Third, many know that cytotoxic chemotherapy causes significant systemic side effects. In contrast, many immunotherapies have relatively favorable tolerability profiles. For example, DC vaccination is usually associated only with mild local or flu-like reactions. This allows patients to maintain quality of life during treatment.
Last but not least, IT can be layered onto standard modalities without overlapping toxicity. For example, CAR-T and ICIs are being combined with radiotherapy or tumor-treating fields (TTFields) to enhance efficacy while maintaining tolerability.
Limitations of Immunotherapy in Germany
Regarding the limitations of immunotherapy (IT) approaches, we should note that these remain among the most expensive treatments in oncology. In Germany, dendritic cell vaccination typically costs €20,000-€38,000. On the other hand, CAR-T programs for solid tumors are estimated at €450,000-€550,000 per patient episode.
Moreover, IT is currently offered primarily at major university hospitals and specialized research centers (e.g., Freiburg, Ulm, Mannheim). The reason is that complex cell therapy manufacturing requires advanced infrastructure. However, unfortunately, smaller regional clinics generally do not have it.
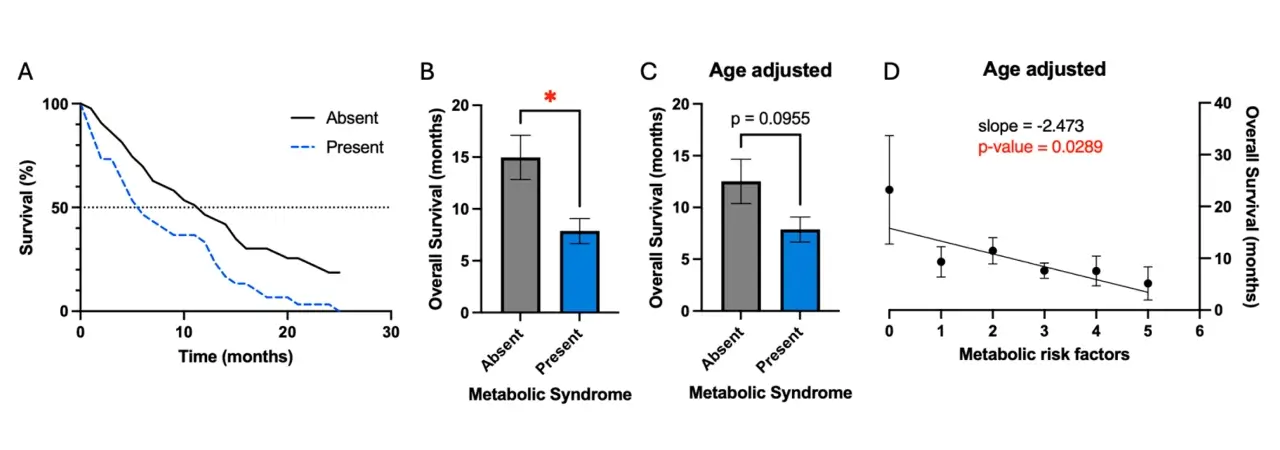
Furthermore, not every patient can develop a strong immune response to vaccination or CAR-T infusion. As we discussed in detail, GBM's immunosuppressive microenvironment, use of steroids, and heterogeneous antigen expression mean that therapeutic efficacy can vary among patients depending on their unique factors. Some patients can achieve long survival. However, others might show only transient responses.
An important aspect of successful therapy is taking into account the general state of health of the patient, in particular, the presence of metabolic syndrome. Statistical analysis shows that concomitant metabolic disturbances can significantly affect life expectancy after the first operation. The graphs below show the relationship between metabolic risk factors and overall survival:
Who Benefits Most?
- Newly diagnosed GBM patients who undergo gross total resection and start IT soon after standard chemoradiation appear to benefit most.
- Recurrent GBM cases may also be considered, especially for experimental IT such as CAR-T or oncolytic viruses.
- Patients with good performance status, minimal steroid dependence, and adequate organ function are generally prioritized for IT programs.
Choosing Clinics for Glioblastoma Immunotherapy in Germany
Choosing a medical facility to treat an aggressive brain tumor is a strategic decision that directly affects the prognosis. Glioblastoma immunotherapy Germany offers provides high standards of treatment through a combination of academic research and practical experience from leading university clinics.
When choosing a medical institution, you should focus on advanced centers specializing in GBM immunotherapy. Clinics in Germany offer access to innovative protocols and a multidisciplinary approach that is critical for successful treatment. But it is also worth paying attention to the following factors:
- Multidisciplinary oncologic tumor board:The best results are achieved where the treatment plan is developed jointly by neurosurgeons, oncologists, radiologists, and immunologists. Only this approach allows the planning of complex care. Advanced glioblastoma treatment immunotherapy give hope for long-term overall survival and become an organic part of the strategy to combat the disease, strengthening the effect of standard protocols.
- Molecular diagnostics and testing:A modern clinic must have its own laboratory for advanced genetic tumor sequencing. This detects specific tumor mutations and selects the most effective glioblastoma treatment options. Immunotherapy, adapted to the biological profile of a specific patient, provides the maximum targeted effect on cancer cells.
- Availability of combined treatment:The clinic must have a technical base for simultaneous immunotherapy, radiation therapy, and electric field treatment (TTFields). It is the synergy of methods that today demonstrates the best survival statistics.
Germany offers not just separate procedures, but a comprehensive system where treatment in Germany becomes part of the patient's holistic path to recovery. By choosing a clinic, you choose the level of technology and expertise, which today is one of the highest in the world.
The three criteria above — tumor board composition, molecular diagnostics infrastructure, and TTFields capability — are not equally present across all German centers.
Booking Health's center matching for GBM is conducted at that level of distinction — not at the level of which centers offer immunotherapy in general, but which center's specific infrastructure and protocol design match the combination approach this patient's clinical situation requires.
FIND THE RIGHT SPECIALIST FOR MY CASECost of Glioblastoma Immunotherapy
For many patients and their families, the issue of cost is one of the crucial ones when choosing a treatment center. In addition to the price itself, time becomes a critical factor: in many countries with a state insurance system, waiting for innovative therapy can last for months. With such an aggressive diagnosis as glioblastoma, this time is often an unacceptable luxury, so patients increasingly choose the advanced GBM immunotherapy. Cost in Germany remains transparent about these procedures, and the technologies themselves have long been integrated into the daily clinical practice of leading centers.
When considering the financial component, it is important to compare different types of treatment. For example, dendritic cell therapy in Germany costs between €20,000 and €38,000, making it significantly more affordable compared to the US, where the price of similar protocols can reach €100,000 – €150,000. Given these numbers, the optimal choice for many is glioblastoma immunotherapy. Cost in Germany often turns out to be more profitable and competitive, especially given the high qualifications of German specialists and access to the latest medical developments.
As for high-tech CAR T-cell therapy, it is one of the most expensive methods in the world. In the US, the cost of such a course varies between €600,000 – €700,000, while in German centers it is approximately €450,000 – €550,000. Most patients, especially foreign ones, choose advanced centers specializing in glioblastoma immunotherapy. Clinics in Germany offer transparent pricing and comprehensive service packages that include not only the drug itself, but also guaranteed long-term medical support, which continues even after the completion of the main course of treatment.
In addition to cellular technologies, monoclonal antibody therapy, which helps the immune system recognize and block specific proteins on the surface of tumor cells, occupies an important place in the protocols. If we consider the cost of this method, in Germany, it is approximately €375,000 – €420,000 for the full course. In the UK, the price for a similar treatment varies between €400,000 – €500,000, while in the US, costs are traditionally higher – from €600,000 to €1,000,000 for the full course. In Australia, the availability is questionable. Such figures confirm that the German medical system offers one of the best ratios of price and access to high-tech medical drugs.
Below is a summary table that allows you to compare the financial costs and the actual availability of immunotherapy methods in different countries of the world.
Comparative review of treatment cost and availability
| Country | Dendritic cell therapy | CAR T-cell therapy | Monoclonal antibodies | Availability of methods |
|---|---|---|---|---|
| Germany | €20,000 – €38,000 | €450,000 – €550,000 | €375,000 – €420,000 for the full course | High (available at profile centres) |
| USA | €100,000 – €150,000 | €600,000 – €700,000 | €600,000 – €1,000,000 for the full course | High (but very high cost) |
| UK | Not available | €400,000 – €600,000 | €400,000 – €500,000 for the full course | Limited |
| Australia | Not available | €550,000 – €700,000 | Availability is questionable | Average (depends on region) |
Germany's DC therapy range is the most accessible entry point in this table — and for UK and Australian patients, it is not the affordable option but the only option, since the therapy is unavailable at home entirely.
Patients coordinating through Booking Health access Germany's prices directly, without the additional fee that clinics apply to international patients.
CHECK IF A BETTER SOLUTION EXISTS FOR YOUProf. Frank Gansauge on Dendritic Cell Therapy
To help our readers see the incredible potential of dendritic cell therapy, we would like to invite you to watch this video interview with Professor Frank Gansauge, head of LDG Laboratories in Germany. He has been working with dendritic cell therapy since 2001, when his clinic became one of the first private laboratories to apply this innovative method. Professor Gansauge describes dendritic cells as the "officers" of the immune system, capable of training effector lymphocytes to attack malignant cells.
In his practice, DC therapy is often combined with chemotherapy or radiation. He reports that this approach can significantly reduce relapse rates and improve survival in cancers (e.g., colon, pancreatic, and more recently glioblastoma).
According to Professor Gansauge, clinical results show that dendritic cell therapy can prolong life expectancy with minimal side effects. In fact, this strategy can prevent tumor recurrence. Yet, he emphasizes that this approach is not a replacement for standard therapies; it is a great complementary tool.
Please watch this video interview with Professor Gansauge to learn more about his experience with dendritic cell therapy. We hope you might find answers to your questions related to the use of this treatment strategy to manage various cancers, including GBM.
VIDEO
How Dendritic Cell Therapy is Transforming Modern Cancer Treatment
Dendritic Cell Therapy
BOOK CONSULTATION
Patient Story: Glioblastoma Immunotherapy in Germany
In January 2024, Daria was diagnosed with glioblastoma (GBM) type IV after emergency surgery for a seizure. She was told that the disease would almost certainly recur. However, her family decided not to give up and started researching options beyond Ireland. They found Booking Health and were connected with Professor Frank Gansauge's team (LDG Laboratories) in Germany.
The reason why Daria and her family decided to try DC therapy is that the concept of this approach felt logical to them – to use dendritic cells to "teach" the immune system to recognize tumor cells. Within 3-4 weeks post-op, Daria traveled to Germany, where she received a personalized dendritic cell vaccine. She then completed standard chemoradiation at home.
Daria experienced no notable side effects from the vaccine. On the contrary, she sustained her energy during chemoradiation. However, what she and her family found most incredible is that her MRI scans at ~3 and ~9 months post-surgery (2024) were clear.
The family believes that early timing and the combined approach (standard care plus DC therapy) were essential. "Don't lose hope. Go early and quickly. Combine standard treatment with dendritic cells if you're eligible."
We invite you to watch this video interview to hear Daria and her husband describe the decision, the procedure, and life after treatment.
VIDEO
Daria Rogers, Ireland:
How Modern Cancer Treatment
in Germany Changed
My Glioblastoma Prognosis
Dendritic Cell Therapy
FIND THE RIGHT SPECIALIST FOR MY CASE
When Canadian doctors told Ron Czenczek his glioblastoma grade IV tumor would not shrink — only, at best, be held in place — his wife Freya began looking for someone who would give them a different answer. Months of high-dose chemotherapy and radiation had already taken everything: his hair, his appetite, the energy to leave the couch. That is what standard treatment costs a body already fighting a grade IV tumor — and his oncologists had nothing left to offer beyond more of it.
Three independent physicians, when asked for alternatives, pointed Freya toward Germany; through Booking Health, she reached Prof. Gansauge's team within days of her first inquiry. The dendritic cell procedure required no hospitalization. A brief low-grade fever followed — not a side effect to manage, but a clinical signal: the immune system had recognized its target and responded. Two subsequent MRIs showed the tumor was smaller — the outcome Ron's Canadian doctors had explicitly said would not occur. Watch the video below to hear him describe what it means to outlive the limit you were given.
VIDEO
Glioblastoma Grade 4: How Dendritic Cell Therapy in Germany Shrank Ronald’s "Terminal" Tumor
Dendritic Cell Therapy
BOOK CONSULTATION
A Medical Journey: Every Step of the Way With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for already 12 years, Booking Health possesses solid expertise in creating complex cancer management programs in each case. As a reputable company, Booking Health offers personalized glioblastoma multiforme treatment plans with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment.
We provide:
- Assessment and analysis of medical reports
- Development of the medical care program
- Selection of a suitable treatment location
- Preparation of medical documents and forwarding to a suitable clinic
- Preparatory consultations with clinicians for the development of medical care programs
- Expert advice during the hospital stay
- Follow-up care after the patient returns to their native country after completing the medical care program
- Taking care of formalities as part of the preparation for the medical care program
- Coordination and organization of the patient's stay in a foreign country
- Assistance with visas and tickets
- A personal coordinator and interpreter with 24/7 support
- Transparent budgeting with no hidden costs
Health is an invaluable aspect of our lives. Delegating management of something so fragile yet precious should be done only to experts with proven experience and a reputation. Booking Health is a trustworthy partner who assists you on the way of pursuing stronger health and a better quality of life. Contact our medical consultant to learn more about the possibilities of personalized treatment with innovative methods for glioblastoma with leading specialists in this field.
Booking Health holds ISO 9001 quality certification, reflecting well-established processes and strict quality control at every stage of the treatment journey — not just at the initial consultation, but throughout.

Every Patient Has a Story: Booking Health Treatment Journeys that Inspire










FAQ: Glioblastoma Immunotherapy in Germany
The method of treatment that activates the patient's own immune system is immunotherapy. Glioblastoma multiforme is attacked by cells of the body itself, which learn to recognize and destroy the tumor.
German centers offer dendritic cell vaccines, checkpoint inhibitors, monoclonal antibodies, and CAR T-cell therapy. Immunotherapy brain tumor protocols in leading hospitals in Germany may also include oncolytic viruses.
Yes, glioblastoma immunotherapy Germany programs provide treatment which significantly prolongs survival, especially when combined with standard protocols.
At the current stage of the development of medicine, immunotherapy is considered a tool for transferring the disease into a state of long-term and stable remission. Full recovery remains a difficult task, but immune activation methods give patients real chances for a long-term life.
CAR T cell therapy can modify a patient's T-cells to target GBM antigens. It is considered one of the most advanced T-cell therapies. The typical CAR T glioblastoma cost in Germany ranges from €450,000-€550,000.
This therapy is one of the most promising areas for patients with specific tumor antigens, as it provides an attack directly on the focus of the disease. Due to the ability of modified T-cells to overcome the defense mechanisms of cancer, this method becomes a strong chance for patients with recurrent forms of glioblastoma, when traditional methods are already exhausted.
Yes, the synergy of methods is considered, because radiation and chemotherapy help release tumor antigens, making it vulnerable to immunity. This combination allows for attacking the disease simultaneously from different angles, increasing the overall effectiveness of the treatment.
Side effects usually include fatigue, flu-like symptoms, or specific inflammatory reactions that arise from the activation of the body's defenses. However, these reactions are usually much easier than the systemic effects of chemotherapy and are effectively controlled by experienced oncologists.
Booking Health glioblastoma immunotherapy support covers medical review, program design, clinic booking, visas, interpretation, and follow-up, among other needs of GBM patients. It ensures transparent costs and efficient access to innovative cancer treatment in leading German centers.
In modern clinics, standard treatment is supplemented by the use of tumor treating fields. Glioblastoma is more effectively controlled due to the effect of these fields on the mitosis of cancer cells, which, in combination with immunotherapy, creates a powerful barrier against the progression of the disease.
Programs differ in the type of immunotherapy. Immune checkpoint inhibitors should be administered within a few months, while dendritic cell therapy is a single injection.
Stage 4 glioblastoma is characterized by headache, nausea, impaired vision, speech, coordination, personality changes, and seizures. Symptoms appear due to rapid tumor growth, pressure on neighboring areas of the brain, and swelling of tissues.
The cost of treatment depends on the method. Monoclonal antibodies cost an average of €375,000 – 420,000, CAR T-cell therapy costs €450,000 – 550,000, and dendritic cell vaccines cost €20,000 – 38,000. Prices are generally higher in the UK and the US, while access to these treatments is still limited in Australia.
Stage 4 glioblastoma has a response rate of around 20% with standard treatment, while the response rate is up to 60% when immunotherapy is added. This approach significantly prolongs disease-free survival and improves overall survival.
Monoclonal antibody therapy provides high specificity of action – drugs recognize tumor cells by unique targets (EGFR, VEGF-A, PD-1/PD-L1) and destroy them. This method is well tolerated and is often combined with chemotherapy or radiation therapy to achieve better results.
CAR T-cell therapy activates the patient’s own immune system, allowing modified cells to recognize and destroy the tumor. Treatment is carried out only in highly specialized clinics and shows a stable, long-term immune effect even in aggressive forms of glioblastoma.
Dendritic cell therapy stimulates natural anti-cancer immunity, prevents relapses, and helps control the tumor process. Its effectiveness is confirmed by clinical observations – patients demonstrate long-term remission and better recovery after basic treatment.
There is no single best treatment for glioblastoma. But for many patients, immunotherapy gives hope. This includes immune checkpoint inhibitors, cellular therapies, dendritic vaccines, or oncolytic viruses – depending on molecular profile and prior treatment response.
Patients can find clinics among the largest university centers in Heidelberg, Munich, Cologne, and other cities. These institutions have their own research institutes and laboratories for the manufacture of individual immune drugs directly within the hospital.
The research institute with a powerful base of neuro-oncology is exactly the best hospital for glioblastoma immunotherapy. Treatment here involves a full cycle of medical support: from determining the feasibility of immune methods to risk management and accurate adjustment of therapy based on regular examinations.
Germany offers structured access to glioblastoma immunotherapy within specialized centers – patients benefit from regulated protocols and experienced neuro-oncology teams. Also, advanced immune-based treatments are available (used under strict clinical supervision).
Choose treatment abroad and you will for sure get the best results!
Sources:
01. Stefaan W Van Gool, Jennifer Makalowski, Linde F C Kampers et al. Dendritic cell vaccination for glioblastoma multiforme patients: has a new milestone been reached? Transl Cancer Res. 2023 Jul 28;12(8):2224–2228. doi: 10.21037/tcr-23-603. [DOI] [PMC free article]
02. Ljupcho Efremov, Semaw Ferede Abera, Ahmed Bedir, Dirk Vordermark, Daniel Medenwald. Patterns of glioblastoma treatment and survival over a 16-years period: pooled data from the German Cancer Registries. J Cancer Res Clin Oncol. 2021 Mar 20;147(11):3381–3390. doi: 10.1007/s00432-021-03596-5. [DOI] [PMC free article]
03. Zouina Sarfraz, Arun Maharaj, Vyshak Alva Venur et al. Immunotherapy in Glioblastoma: An Overview of Current Status. Clin Pharmacol. 2025 Jul 24;17:185–209. doi: 10.2147/CPAA.S497903. [DOI] [PMC free article]
04. Aleksandra Królikowska, Maciej Tarnowski. CAR-T cells immunotherapy in the treatment of glioblastoma. Cancer Immunol Immunother. 2025 Nov 6;74(12):363. doi: 10.1007/s00262-025-04222-w. [DOI] [PMC free article]
05. Merve Hazal Ser, Mason J Webb, Ugur Sener, Jian L Campian. Immune Checkpoint Inhibitors and Glioblastoma: A Review on Current State and Future Directions. J Immunother Precis Oncol. 2024 May 2;7(2):97–110. doi: 10.36401/JIPO-23-34. [DOI] [PMC free article]
06. Damir Nizamutdinov, Anna Sentmanat, Jing Tong et al. The Emerging Role of Oncolytic Virotherapy in Glioblastoma Management. Cancers (Basel). 2025 Oct 28;17(21):3465. doi: 10.3390/cancers17213465. [DOI] [PMC free article]
07. Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x. [DOI] [PubMed]
08. Linda M Liau, Keyoumars Ashkan, Steven Brem et al. Association of Autologous Tumor Lysate-Loaded Dendritic Cell Vaccination With Extension of Survival Among Patients With Newly Diagnosed and Recurrent Glioblastoma. JAMA Oncol. 2022 Nov 17;9(1):112–121. doi: 10.1001/jamaoncol.2022.5370. [DOI] [PMC free article]
09. Duan M, Cao R et al. Blood-Brain Barrier Conquest in Glioblastoma Nanomedicine: Strategies, Clinical Advances, and Emerging Challenges. Journals. Cancers. Volume 16. Issue 19. doi:10.3390/cancers16193300. [DOI]
10. Aboubechara JP, Aboud O. Metabolic Risk Factors and Survival in Patients with Glioblastoma. Journals. Cancers. Volume 16. Issue 21. doi: 10.3390/cancers16213666. [DOI]
11. Liu J, Wang Yu et al. Oncolytic Viruses in Glioblastoma: Clinical Progress, Mechanistic Insights, and Future Therapeutic Directions. Journals. Cancers. Volume 17. Issue 24 doi: 10.3390/cancers17243948. [DOI]
Read: