A cancer diagnosis changes everything. Yet colon cancer – one of the most common malignancies worldwide – has never been more treatable, more understood, or more responsive to innovation than it is today. After treatment for colon cancer stage 1, patients achieve five-year survival rates of 90% [1], while even advanced cases now benefit from targeted drug delivery, immunotherapy, and precision tumor destruction techniques that barely existed a decade ago. The goal isn't just survival – it's quality of life, restored.
Understanding Colon Cancer: Key Facts About This Disease
Nearly 2 million new cases emerge globally each year [2]. In the United States alone, over 107,000 Americans will receive a colon cancer diagnosis in 2025 – men and women affected in almost equal measure [3]. Daunting numbers, certainly. But here's what those statistics don't capture: this disease responds extraordinarily well to early detection.
Screening changes outcomes. For adults over 50 – or earlier when family history is a factor – regular screening catches precancerous polyps before they transform into cancer altogether. Localized disease, caught before it spreads beyond the bowel, achieves surgical cure rates of approximately 50%. The window of opportunity is real, and it's wide.
Advanced cases demand more: specialized expertise and multimodal strategies (for a patient's specific condition).
Conventional Treatment Approaches for Colon Cancer
Surgery forms the cornerstone of treatment of colon cancer [4] – removing the tumor and surrounding lymph nodes, then building outward from there. Additional therapies layer on based on disease stage and the patient's overall condition. The logic of colon cancer treatment by stage is straightforward. The execution varies enormously.
Bowel cancer treatment at stage 1 keeps things relatively contained. Very small cancers may be addressed through polypectomy during colonoscopy; larger polyps call for endoscopic mucosal resection; more complex cases move to minimally invasive laparoscopic surgery—with shorter hospital stays and faster recovery than traditional open procedures. Surgery, and done. No chemotherapy or radiation.
Stage 2 colon cancer treatment shifts the approach. A partial colectomy removes the tumor-containing bowel segment along with a margin of healthy surrounding tissue – and for select high-risk patients, adjuvant chemotherapy follows, targeting any microscopic residual cells that surgery couldn't guarantee it caught.
Treatment for stage 3 colon cancer raises the stakes entirely: surgical resection combines with adjuvant chemotherapy to pursue cancer cells that may have already migrated to nearby lymph nodes. The goal: cut recurrence risk before it becomes recurrence reality.
Stage 4 is where treatment becomes genuinely multimodal. Surgery (when indicated), systemic chemotherapy, targeted therapies attacking specific tumor markers, and new treatment for colon cancer stage 4, immunotherapy activating the body's own defenses – sometimes all of the above. When surgery isn't an option, radiation addresses symptoms directly.
Four stages. Four distinct strategies. Precision isn't optional here – it's the entire point.
Advanced Intraperitoneal Chemotherapy Methods for Colon Cancer
Peritoneal metastasis – cancer spreading to the abdominal lining – presents a specific challenge. Standard intravenous chemotherapy struggles to reach these surfaces in meaningful concentrations. The solution? Deliver the drugs directly.
Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Colon Cancer
HIPEC is considered a significant advance and new treatment for colon cancer with peritoneal spread [5]. It doesn't choose between surgery and chemotherapy – it combines them, sequentially and precisely, in a single procedure designed to address what surgery alone cannot.
The mechanism is elegant. Where systemic chemotherapy barely penetrates peritoneal surfaces, HIPEC circulates heated drug solution – at temperatures between 40 and 43°C – directly throughout the abdominal cavity after surgical tumor removal. Heat amplifies drug absorption. [9] Direct contact eliminates the delivery barrier entirely. The result: chemotherapy concentrations up to 15 times higher than traditional methods, reaching microscopic cancer cells invisible to the surgeon's eye, while the rest of the body experiences far less toxic burden.
What does the procedure actually involve? First, cytoreductive surgery – meticulous removal of every visible tumor deposit from the peritoneal surfaces. Once complete, specialized drains are positioned throughout the cavity, and heated chemotherapy solution circulates for 30 to 90 minutes through a precision perfusion system ensuring even distribution. The entire process runs 5 to 10 hours. Recovery requires 10 to 14 days in the hospital.
Demanding? Yes. But for patients with peritoneal metastasis, HIPEC offers something conventional treatment often cannot: meaningful life expectancy extension, with genuine therapeutic impact.
HIPEC's survival benefit applies to patients who were correctly selected — those with limited peritoneal disease burden, adequate performance status, and no extra-abdominal metastases. Peritoneal carcinomatosis index, prior surgical history, and organ function all factor into eligibility.
Booking Health evaluates each patient's imaging before travel is organized, so that the first appointment is a treatment planning session rather than an eligibility determination.
For a deeper understanding of this approach, watch our exclusive interview with Dr. Michael Lipp – a leading HIPEC specialist – as he explains how the procedure is reshaping outcomes for patients facing peritoneal spread.
VIDEO
Dr. Michael Lipp on HIPEC Treatment: A Breakthrough in Advanced Abdominal Cancer Care
General and Abdominal Surgery, Hepatopancreatobiliary Surgery and Hernia Surgery
Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for Colon Cancer
Not every patient can tolerate major surgery. For those with peritoneal metastases who can't – PIPAC offers something different. [6]
Where HIPEC demands extensive surgical intervention, PIPAC works through just two small abdominal incisions. Liquid chemotherapy is transformed into pressurized aerosol, distributed throughout the abdominal cavity under pressure, held for 30 minutes, then removed. The entire procedure runs 60 to 90 minutes. Recovery? Days, not weeks – sometimes outpatient entirely, otherwise a 2-3 day hospital stay versus the 10-14 days HIPEC requires.
What makes PIPAC particularly valuable is its repeatability. Every 6-8 weeks, treatment can be administered again – managing disease progression over time rather than attempting a single definitive intervention. It runs concurrently with systemic chemotherapy, suits patients too frail for aggressive surgery, and carries minimal physical trauma throughout. Perhaps most significantly, PIPAC can downstage disease: shrinking and stabilizing tumors enough that more aggressive surgical options become viable later.
The core problem it solves is drug delivery. Systemic chemotherapy struggles to penetrate peritoneal surfaces effectively – PIPAC bypasses that barrier entirely through direct aerosolized contact. For patients with extensive peritoneal spread who aren't HIPEC candidates, that distinction matters enormously.
A bridge therapy, in the truest sense. One that keeps treatment active while protecting quality of life.
PIPAC's 6-8 week cycle creates a specific coordination requirement for international patients: between sessions, peritoneal carcinomatosis reassessment must reach the German treating team so each subsequent session is planned on current rather than outdated disease burden.
Booking Health's personal coordinator maintains that information channel throughout the full treatment course — translating interim imaging reports and relaying them to the German team before each scheduled session.
Transarterial Chemoembolization for Colon Cancer: Targeted Liver Metastases Treatment
When colon cancer spreads to the liver and surgery isn't viable, TACE steps in – a precision therapy that turns the tumor's own biology against it. Everything starts with anatomy.
The human liver normally receives blood from two sources: the portal vein supplies healthy tissue, and the hepatic arteries feed tumors, almost exclusively. Thread a catheter through a small groin incision, navigate to hepatic arteries, reach the vessels feeding the metastases – and suddenly, the tumor's dependency becomes its vulnerability.
The treatment delivered through that catheter does two things at once. Embolic materials physically block the artery, cutting off blood flow and starving cancer cells of oxygen and nutrients. Chemotherapy – trapped, concentrated, unable to disperse – saturates the tumor at levels up to 20 times higher than anything systemic IV delivery could achieve. [10] No dilution through the bloodstream. No systemic spread. Just sustained, direct contact between the drug and the cancer cell, for far longer than conventional methods allow.
Healthy liver tissue? It draws from different vessels. It largely escapes the process entirely.
What does this mean for a patient? Recovery measured in hours, not weeks – most patients are home within 24-48 hours. Side effects a fraction of standard chemotherapy, because the drugs stay local rather than circulating through the entire body. Treatment is repeatable (every 4-6 weeks), adjusted as the disease evolves, with liver function preserved throughout.
For patients for whom surgery can no longer help – or whose disease has stopped responding to systemic chemotherapy – TACE reframes what treatment can look like. Not a compromise. A genuinely different mechanism, with meaningful results.
The choice between DEB-TACE and conventional TACE — the subject of Prof. Kovács's interview — depends on tumor vascularity, hepatic reserve, and whether prior treatment has altered the vascular feeding pattern of the hepatic metastases.
Booking Health identifies which centers have documented volume in both techniques and maps each patient's hepatic disease burden to the center whose interventional radiology team has the specific procedural experience the case requires.
VIDEO
Prof. Kovács: Why Interventional Oncology Should Be the Fourth Pillar of Cancer Care
Built on Nobel Prize-winning science[7], this approach reprograms the body's own immune cells to recognize and target a patient's specific colon cancer. The process begins simply – a blood draw, similar to donation, harvests dendritic cells that are then processed in GMP-certified laboratories. There, they're "educated" using proteins from the patient's own tumor, essentially creating a personalized vaccine calibrated to that individual's cancer characteristics.
Once reinfused, these reprogrammed cells activate T-cells throughout the body – generating targeted anti-cancer immunity that pursues malignant cells wherever they've spread. Not just at the primary site. Everywhere.
The side effect profile is mild: primarily flu-like symptoms lasting one to two days. What is important, treatment is compatible with surgery, chemotherapy, and other concurrent therapies. It suits patients too frail for aggressive interventions, preserves daily function, and – crucially – continues working after treatment ends, building lasting immunity rather than a temporary response.
European cancer centers report meaningful outcomes with immunotherapy for bowel cancer: disease stabilization, reduced tumor burden, extended survival, and sustained quality of life improvements across both 4 stage colorectal cancer treatment and earlier-stage patients. For those for whom conventional treatment has failed, it represents a fundamentally different mechanism of attack.
Surgery isn't always the answer. For patients with liver or lung metastasis who can't tolerate major procedures, thermal and freezing technologies destroy tumors through an entirely different means – controlled heat or extreme cold, delivered precisely, with same-day discharge and minimal disruption to daily life.
Thermal Ablation Techniques: RFA and Microwave Technology
Two technologies dominate thermal ablation for colon cancer liver metastases – radiofrequency ablation (RFA) and microwave ablation (MWA). Both destroy tumor tissue through heat. Their mechanisms, and their strengths, differ. [8]
RFA inserts a thin needle directly into the tumor under imaging guidance, delivering high-frequency electrical current that heats the site to between 60 and 100°C. Ten to fifteen minutes per tumor, effective for lesions up to 5cm. Straightforward, well-established, with a strong complication-rate profile.
MWA uses electromagnetic energy instead – generating friction-based heat that destroys tissue faster, in 5 to 13 minutes, and performs reliably even near major blood vessels where RFA loses effectiveness. Newer, quicker, better suited to complex anatomical locations.
Both procedures are outpatient. Both can be repeated as new metastases develop. Both carry lower complication rates than surgical resection and work across liver and lung metastases alike – making them genuinely practical options for patients managing advanced pathology while protecting what matters most: the ability to keep living normally.
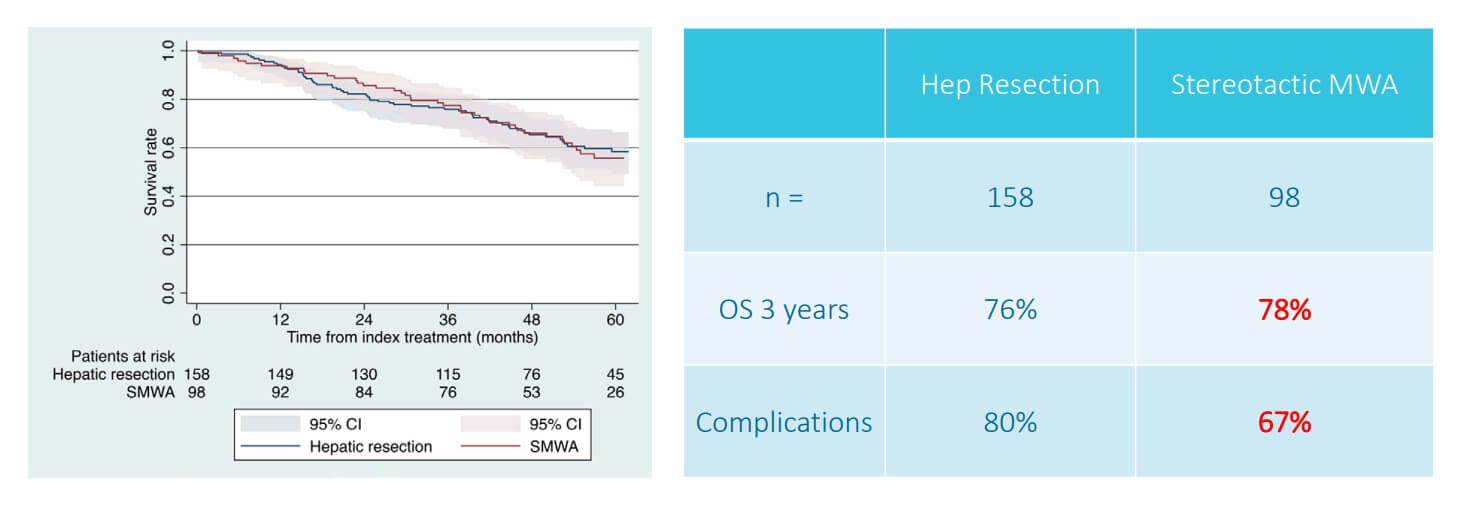
A prospective multicentre trial on survival after Microwave Ablation VErsus Resection for Resectable Colorectal liver metastases (MAVERRIC)
Cryotherapy for Colon Cancer: Eliminating Tumors Through Controlled Freezing
Extreme cold destroys. Cryoablation turns that principle into a natural treatment.
Using liquid nitrogen to drive temperatures below -75°C, specialized probes inserted directly into tumors create an expanding "ice ball" that engulfs cancer tissue – rupturing cell membranes, triggering natural cell death, and leaving surrounding structures largely intact. The area is frozen, thawed, then frozen again, ensuring complete destruction throughout. Both liver and lung metastases respond to the technique.
Key advantages for colorectal cancer patients include:
Exceptional visibility of treatment boundaries during the procedure
Precise control between treated and healthy tissue
Effective near blood vessels and critical structures
Treatment of tumors up to 4cm in diameter
Can be performed through open surgery, laparoscopy, or percutaneously
The procedure suits patients with multiple tumors across both liver lobes, lesions in surgically inaccessible locations, or individuals too high-risk for major operations. Recovery runs 3-4 days in hospital. Post-procedural pain is typically minimal.
RFA, MWA, and cryoablation are not interchangeable for the same lesion. Tumor size, proximity to hepatic vessels, and prior treatment all point to different modalities — and centers offering one or two of these techniques will recommend from their available menu rather than from the tumor's characteristics.
Booking Health maps each patient's metastatic pattern and imaging against the documented procedural capabilities of candidate German centers, identifying which institution has the specific ablation expertise the case requires.
Mostly mild effects (mainly limited to temporary discomfort at the treatment site)
Cost in Germany
€80,000 - €150,000 full course
€25,000 - €60,000 full course
Cost in Great Britain
€90,000 - €165,000 full course
€70,000 - €120,000 full course
Cost in the USA
€100,000 - €180,000 full course
€100,000 - €150,000 full course
The 60% two-year survival in the innovative methods column applies to correctly matched patients — those whose peritoneal carcinomatosis index qualifies them for HIPEC, whose hepatic disease burden and vascularity suit TACE, whose MSI status supports immunotherapy.
Booking Health's case review determines which specific method a patient's imaging, molecular profile, and functional status support — provided within 24 hours of receiving the clinical record, by a physician who has reviewed the actual case.
Fear was the first response. When Sarasibala Premachandran received a stage 4 colon cancer diagnosis in Britain, her daughter Sughandi describes the weight of that moment – and the determination that followed it.
The family refused to stop at limited local options. Research led them to the University Hospital Frankfurt am Main in Germany, to Prof. Vogl's specialized care – and to a decision that felt enormous at the time.
"We were nervous about traveling abroad for new colon cancer treatment, especially with mum being so unwell," Sughandi recalls. "But from the moment we arrived, we felt supported and informed."
Sarasibala underwent TACE – transarterial chemoembolization – delivering concentrated chemotherapy directly to tumor sites while cutting off their blood supply. A dedicated coordination team bridged communication between the family and medical staff throughout the three-week program, smoothing a process that could easily have felt overwhelming from abroad.
"Dr. Vogl has been amazing – knowledgeable, understanding, and trustworthy," Sughandi notes. "We're nearly at the end of our journey here and feeling very hopeful about the results."
Through specialized expertise and care that extended beyond the clinical, patients receive many more benefits.
Best Clinics for Bowel Cancer Treatment
5 German university hospitals have decades of specialized expertise and cutting-edge technology. These bowel cancer specialist hospitals integrate multiple innovative approaches and prices can sometimes be comparable to bowel cancer private treatment cost.
University Hospital of Ludwig Maximilian University of Munich
The Comprehensive Cancer Center Munich works on the basis of the University Hospital of Ludwig Maximilian University of Munich – with 3,500 beds dedicated to oncology. What sets this center for colon cancer apart? Volume and precision. Over 3,500 patients visit the Department of Gastroenterology and Hepatology annually. Surgeons here use laparoscopic techniques that minimize tissue trauma – which explains why Focus magazine consistently names this facility Germany's best hospital for bowel cancer treatment.
Asklepios Hospital Barmbek Hamburg
Hamburg's contribution comes from an unexpected source: a relatively young facility established in 2005. Asklepios Hospital Barmbek Hamburg, with just 620 beds, is the academic hospital of the University of Hamburg, and ranks among the world's top three medical tourism centers according to MTQUA standards. Not bad for a newcomer. Prof. Dr. Michael Lipp performs HIPEC procedures here weekly – cytoreductive surgery paired with heated intraperitoneal chemotherapy – and the hospital for best colon cancer treatment designation reflects both surgical prowess (36,000 inpatients yearly) and patient satisfaction scores that consistently exceed European benchmarks. ISO 9001:2015 certification and German Cancer Society accreditation validate the hospital’s work.
University Hospital RWTH Aachen
Maximum care requires maximum resources. University Hospital RWTH Aachen delivers both: over 60 departments, 940+ physicians, approximately 95 professors. Its Department of General, Abdominal, Transplant Surgery performs 3,000+ operations annually. That volume translates directly to surgical proficiency. Four high-tech operating rooms feature CUSA and LIMAX systems that influence bowel cancer surgery cost, offer minimally invasive procedures – these make this bowel cancer clinic valuable for patients with peritoneal or liver metastases requiring HIPEC or chemoembolization (TACE).
University Hospital Düsseldorf
Scale matters in oncology. University Hospital Düsseldorf helps 50,000+ inpatients and 300,000+ outpatients yearly. Its certified Center for Treatment of Bowel Diseases is supported by 10 specialized outpatient clinics – addressing everything from diagnostic colonoscopy to follow-up after the treatment program completion. The average cost of colon cancer treatment here remains competitive, with outcomes that match or even exceed international standards.
University Hospital Ulm
University Hospital Ulm is among Germany's best bowel cancer clinics. Its Comprehensive Cancer Center is certified under the standards of the German Cancer Society and ISO 9001:2008. The Department of Gastroenterology and Hepatology focuses on gastrointestinal cancers, treating oncology with the help of endoscopic procedures, comprehensive surgical interventions, and so on. This best clinic for colon cancer treatment also offers innovative CAR T-cell therapy (available only at the most advanced centers worldwide) and holds leading positions globally in bone marrow transplantation. Thanks to this, patients receive tomorrow's treatments today.
What do these colon cancer best treatment centers share? German Cancer Society certification. High surgical volumes exceeding 250 procedures yearly. ISO-certified quality. Yet each brings unique strengths.
Choosing among colon cancer clinics requires weighing multiple factors. The best colon cancer hospital for one patient may differ entirely from another's ideal choice – clinical situation, metastasis pattern, cost of private bowel cancer surgery, personal priorities regarding treatment intensity versus quality of life all influence the decision.
Full surgical spectrum, systemic therapies, radiation therapy
Yes (Center for Bowel Diseases)
University Hospital Ulm
High volume across 29 departments
CAR T-cell therapy, dendritic cell immunotherapy, bone marrow transplant
Yes (DKG + ISO 9001:2008)
Booking Health maintains partnerships with all five facilities, coordinating patient care. International patients can access Germany's best hospital for colon cancer without dealing with complex issues independently.
Those five centers serve genuinely different clinical profiles. LMU Munich for high-volume laparoscopic surgery and gastroenterology-led multimodal planning. Asklepios Barmbek for HIPEC specifically, with Prof. Lipp performing the procedure weekly. RWTH Aachen for complex peritoneal and hepatic disease requiring the full interventional radiology and surgical spectrum simultaneously. Düsseldorf for patients needing comprehensive disease management across the full treatment course with 10 specialized outpatient clinics. Ulm for patients whose tumor biology qualifies them for CAR T-cell therapy or DC vaccination — treatments available only at the most advanced centers. A patient with peritoneal carcinomatosis requiring HIPEC needs a different center than one with hepatic metastases requiring TACE alongside DC vaccination.
Booking Health maps each patient's case to the institution whose specific documented strengths most directly address their clinical situation.
Final costs depend on case complexity, hospital stay duration, required follow-up care, and additional expenses such as diagnostic procedures, travel arrangements, and lodging expenses.
Country
Conventional therapy
Innovative therapy
Cost in Germany
€80,000 - €150,000 full course
€25,000 - €60,000 full course
Cost in Great Britain
€90,000 - €165,000 full course
€70,000 - €120,000 full course
Cost in the USA
€100,000 - €180,000 full course
€100,000 - €150,000 full course
Modern Cancer Treatment: Patient Journeys with Booking Health
Diane O. (United Kingdom), March 2026
Faeqa M. (Bahrain), March 2026
Helen G. (United Kingdom), February 2026
Patrick D. (Ireland), December 2025
Ronald C. (Canada), November 2025
Monica A. (Croatia), October 2025
Robert B. (USA), September 2025
David D. (United Kingdom), September 2025
Sargon B. (USA), August 2025
Amanda Louise C. (Australia), July 2025
Vaidotas Z. (Lithuania), July 2025
Eliza A. (Armenia), June 2025
Margery Sue S. (USA), June 2025
Renewed Hope: What Modern Therapies Promise Patients
Stage 4. Two words that can make the future feel impossibly narrow, but a stage 4 colon cancer treatment isn't the end of options. It's the moment to start looking beyond standard protocols. Modern cancer centers build individualized combinations from a growing arsenal of therapies matched specifically to a patient.
How does that look in practice? TACE targeting liver metastases. Dendritic cell immunotherapy activating the body's own defenses. Minimally invasive ablation techniques destroying tumors without treatment with major surgery. These aren't experimental last resorts – they're established, specialized approaches that standard oncology departments often don't offer, or don't combine effectively.
The difference is significant. Where traditional chemo treatment means weeks of hospitalization and severe side effects, many innovative therapies involve short outpatient visits, minimal disruption to daily life, and meaningful clinical results.
The key – for advanced colon cancer and stage 4 rectal cancer alike – lies in finding centers that provide comprehensive evaluation and multiple treatment options under one roof. Specialized international facilities exist precisely for this: patients whose local options have narrowed, who need expertise concentrated around their specific case rather than a generalized protocol.
Your diagnosis shapes the challenge. It doesn't determine the outcome. The right combination of modern therapies, guided by experienced specialists, can transform even the most difficult prognosis into something manageable – and something worth fighting toward.
Your Trusted Partner: Every Step of the Way With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for 12 years, Booking Health possesses solid expertise in creating complex cancer management programs in each case. As a reputable company, Booking Health offers personalized stage 4 colon cancer treatment plans with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment.
We provide:
Assessment and analysis of medical reports
Development of the medical care program
Selection of a suitable treatment location
Preparation of medical documents and forwarding to a suitable clinic
Preparatory consultations with clinicians for the development of medical care programs
Expert advice during the hospital stay
Follow-up care after the patient returns to their native country after completing the medical care program
Taking care of formalities as part of the preparation for the medical care program
Coordination and organization of the patient's stay in a foreign country
Assistance with visas and tickets
A personal coordinator and interpreter with 24/7 support
Transparent budgeting with no hidden costs
Contact our medical consultants to learn how we can help you begin a personalized, hope-driven approach to brain cancer treatment in Germany or any other country of your choice with some of the world's leading specialists.
Uncontrolled cell growth in the large intestine – that's the simple definition. In practice, it usually begins as small, benign polyps that slowly turn malignant, starting in the inner lining and working deeper through tissue layers if nothing intervenes.
Is colon cancer curable?
Yes – and more reliably than most people assume. Stage 1 cure rates exceed 90%. Advanced cases present greater challenges, but modern therapies have transformed what "advanced" actually means for long-term survival and daily quality of life.
What causes colon (bowel) cancer?
Several factors raise risk: age over 50, family history, inflammatory bowel disease, smoking, high-fat diet. Yet plenty of patients share none of these characteristics. Colon cancer develops across a wide population – which is the strongest argument for screening everyone, not just high-risk groups.
What are the signs of colon (bowel) cancer?
Early disease rarely announces itself. Later warning signs include blood in stool, persistent abdominal pain, unexplained weight loss, shifting bowel habits, and fatigue caused by anemia. The problem: each symptom alone seems explainable. Together, they demand investigation.
Is colon cancer hereditary?
Sometimes. Inherited mutations drive roughly 5-10% of diagnoses. Family history genuinely matters – but most people who develop colon cancer have no genetic predisposition and no family history of the disease at all.
What are the symptoms of colon cancer?
Rectal bleeding and cramping are the most recognizable. Others are subtler – persistent fatigue, narrowing stools, a feeling that the bowel never fully empties. Symptoms that linger beyond a few weeks deserve medical attention. Promptly.
How to detect colon cancer without a colonoscopy?
Stool tests identifying blood or abnormal DNA markers offer a non-invasive starting point. But colonoscopy does something those tests cannot: it removes precancerous polyps during the same procedure, stopping cancer before it starts.
How is colon cancer diagnosed?
Colonoscopy with tissue biopsy confirms diagnosis. From there, CT or MRI scans establish staging, while tumor biomarker blood tests reveal disease extent – together building the complete picture that guides every treatment decision that follows.
How common is colon (bowel) cancer?
Globally, it ranks third among all cancers – nearly 2 million new cases annually. The United States alone expects over 107,000 diagnoses in 2025. Men and women are affected in almost equal measure.
How fast does colon cancer grow?
Most cases develop slowly – the journey from polyp to cancer typically spans 5 to 10 years. That window is precisely why screening works. Some aggressive variants move faster, though. Waiting for symptoms and treatment delay is a gamble not worth taking.
Can colon cancer be cured without surgery?
Small early polyps? Yes – removed entirely during colonoscopy, no further intervention required. For more advanced disease, immunotherapy and other modern approaches increasingly complement conventional treatment for bowel cancer. That said, surgery remains the primary solution for most diagnoses.
What is the survival rate of colon (bowel) cancer?
Localized disease: over 90% five-year survival. Regional spread: around 70%. Distant metastases: approximately 15% – though personalized approaches to treatment of bowel cancer are actively shifting even that figure. Stage at diagnosis remains the single most influential factor.
What are the current treatment guidelines for colon cancer?
Surgery first, chemotherapy added for intermediate and metastatic stages. Increasingly, that framework expands to include precision medicine – treatment decisions built around individual tumor genetics rather than generalized stage-based protocols.
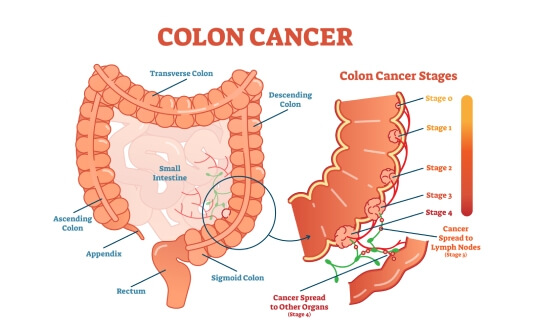
How is colon cancer treated at different stages?
Colon cancer stage 1 treatment needs surgery alone. Stages 2 and 3 pair resection with chemotherapy. Stage 4 demands the full toolkit – targeted therapies, immunotherapy, decisions shaped by the tumor's specific genetic characteristics. One disease, four genuinely different advanced bowel cancer treatment realities.
What is the recommended treatment for stage 1 colon cancer?
Surgical removal of the tumor and surrounding tissue, typically through minimally invasive techniques. Most patients need nothing beyond that – and long-term cure rates reflect it. Clean margins, no further therapy, excellent outcomes.
What are the options for stage 3 colon cancer treatment?
During stage 3 colon cancer treatment, surgical resection combined with adjuvant chemotherapy targets microscopic disease that surgery alone can't guarantee it eliminated. Where tumors are large or complex, neoadjuvant therapy may shrink them first – creating better surgical conditions before the operation begins.
Is chemotherapy always required for colon cancer?
No. Early stages frequently need only surgery. The decision depends on stage, tumor characteristics, and the patient's overall health. For specific cancer profiles, monoclonal antibody therapies offer targeted alternatives to traditional chemotherapy regimens.
What is adjuvant therapy in colon cancer?
Chemotherapy delivered after surgery – not because visible cancer remains, but because microscopic cells might. In intermediate and advanced disease, adjuvant therapy meaningfully reduces the probability that those cells ever become something larger.
What are the latest treatments for colon (bowel) cancer?
Dendritic cell vaccination. HER2-positive tumors and targeted therapies. Genetic testing-driven precision medicine. Thermal ablation with minimal recovery time. The field is advancing rapidly – and the consistent direction is toward greater precision, fewer side effects, better outcomes.
Can colon cancer be treated without surgery?
For patients who can't tolerate major procedures, genuinely effective alternatives exist. Ablation destroys tumors through heat or cold. Chemoembolization targets liver metastases directly. Immunotherapy activates the body's own defenses. Surgery isn't always the only answer – or the right one.
How long is the recovery after colon cancer surgery?
Open surgery: 4-6 weeks typically. Minimally invasive approaches: 2-4 weeks. Full return to normal activity usually follows within 6-8 weeks, with complete internal healing continuing for several months beyond that point.
What is recommended after colon cancer treatment?
Surveillance, consistently. Regular follow-up visits, tumor marker blood tests, imaging scans, colonoscopy monitoring – these aren't optional extras but the infrastructure that catches recurrence early, when it's still manageable. Lifestyle changes – diet, exercise, reduced risk factors – build on that foundation.
What is the two-year survival rate for colon cancer with modern treatments?
The two-year survival rate for colon cancer is around 25% with standard therapy. However, it can reach up to 60% with innovative treatments (e.g., HIPEC, TACE, or dendritic cell immunotherapy).
How do survival outcomes differ between standard and advanced treatment approaches for colon cancer?
Colon cancer patients can achieve longer survival with advanced therapies in comparison to those who are treated with conventional chemotherapy alone.
What treatment response rates are typically seen in colon cancer?
Standard chemotherapy for colon cancer shows response rates below 10%. On the other hand, modern therapies (e.g., dendritic cell therapy) can achieve ~45-65% response.
How long does colon cancer treatment usually take?
Conventional chemotherapy for colon cancer can take several months across multiple cycles. In turn, innovative treatments (e.g., TACE, thermal ablation, etc.) require only a few short sessions.
What are the usual side effects of colon cancer treatment?
Traditional colon cancer treatments (e.g., chemotherapy, radiation, etc.) may cause fatigue, nausea, and hair loss. In comparison, innovative options (e.g., dendritic cell therapy, TACE, ablation, etc.) can lead to mild, temporary discomfort.
How does colon cancer treatment impact everyday life?
Patients with colon cancer treated with advanced therapies usually experience faster recovery. They can continue their normal activities with fewer side effects when compared to those who receive standard chemotherapy.
What are the main treatment options for colon cancer?
Treatment is stage-dependent and multidisciplinary. Approaches such as HIPEC or PIPAC are considered for peritoneal spread; TACE targets liver-dominant disease; dendritic cell therapy may complement standard care by supporting tumor-specific immune response at any stage.
Which hospital provides the most advanced colon cancer treatment?
Centers with dedicated colorectal oncology units and experience in locoregional therapies show the best outcomes. German hospitals offering HIPEC, PIPAC, interventional radiology procedures (like TACE) and personalized immunotherapy (providing comprehensive treatment planning).
Which country is best for colon cancer treatment?
Germany is widely recognized for evidence-based colorectal cancer management. Here specialized centers provide access to advanced treatments within structured clinical pathways.
Choose treatment abroad and you will for sure get the best results!
Authors:
This article was edited by medical experts, board-certified doctors Dr. Nadezhda Ivanisova, and Dr. Bohdan Mykhalniuk. For the treatment of the conditions referred to in the article, you must consult a doctor; the information in the article is not intended for self-medication!
Our editorial policy, which details our commitment to accuracy and transparency, is available here. Click this link to review our policies.
05.Ammerata G, Filippo R, Laface C, et al. Hyperthermic intraperitoneal chemotherapy and colorectal cancer: From physiology to surgery. World J Clin Cases. 2022;10(30):10852-61. doi:10.12998/wjcc.v10.i30.10852.[DOI]
06.Ellebæk SB, Graversen M, Detlefsen S, et al. Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC)-directed treatment of peritoneal metastasis in end-stage colo-rectal cancer patients. Pleura Peritoneum. 2020;5(2):20200109. doi:10.1515/pp-2020-0109.[DOI]
07.Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x.[DOI][PubMed]
08.Ruers T, Punt C, Van Coevorden F, et al. Radiofrequency ablation combined with systemic treatment versus systemic treatment alone in patients with non-resectable colorectal liver metastases: a randomized EORTC Intergroup phase II study (EORTC 40004). Ann Oncol. 2012;23(10):2619-26. doi:10.1093/annonc/mds053.[DOI]
09.Klaver CE, Stam R, Sloothaak DA, et al. Colorectal cancer at high risk of peritoneal metastases: long term outcomes of a pilot study on adjuvant laparoscopic HIPEC and future perspectives. Oncotarget. 2017;8(31):51200-9. doi:10.18632/oncotarget.17158.[DOI]
10.Vogl TJ, Marko C, Langenbach MC, et al. Transarterial chemoembolization of colorectal cancer liver metastasis: improved tumor response by DSM-TACE versus conventional TACE, a prospective, randomized, single-center trial. Eur Radiol. 2021;31(4):2242-51. doi:10.1007/s00330-020-07253-2.[DOI]
11.Tinguely P, Ruiter SJS, Engstrand J, et al. A prospective multicentre trial on survival after microwave ablation versus resection for resectable colorectal liver metastases (MAVERRIC). Eur J Cancer. 2023;187:65-76. https://doi.org/10.1016/j.ejca.2023.03.038.[DOI]
thank you for reaching out! One of our medical advisors is currently reviewing your details. You can expect a call from us within one business day to discuss your request.
Note: The incoming call will appear as a German number or your local area code. This call is entirely free of charge.
Booking Health guarantees:
Expert Placement
We use rigorous statistical analysis to ensure you are treated at the best-rated facility for your specific diagnosis.
Total Cost Protection
No hidden fees or unexpected bills. We provide a fixed price guarantee, backed by insurance that covers any additional complications.
12-Month Extended Care
Your recovery is our priority. Benefit from a full year of direct medical support following your procedure.