Endometrial cancer is the most common gynecologic malignancy in Europe. According to the European Cancer Information System (ECIS), supported by the European Network of Cancer Registries (ENCR), there were approximately 125,000 new cases of endometrial cancer diagnosed across Europe in 2022, accounting for nearly 6% of all female cancers in the region [1].
The disease primarily affects postmenopausal women, with a median age at diagnosis of around 67 years. While early detection rates are relatively high, largely due to symptoms like postmenopausal bleeding, incidence rates have been gradually increasing – a trend largely attributed to rising obesity levels and aging populations, as noted by the European Society for Medical Oncology (ESMO).
Understanding Endometrial Cancer
Endometrial cancer is the most common malignant neoplasm of the female reproductive organs in Europe, which is mainly diagnosed in women after menopause. The incidence continues to increase, making this pathology a significant public health problem and highlighting the importance of timely uterine cancer treatment.
Histological Types of Endometrial Cancer
Two main types are usually distinguished:
Type I (endometrioid adenocarcinoma) – is the most common and less aggressive form. It is estrogen-dependent and often associated with obesity, diabetes and long-term exposure to exogenous estrogens. It is characterized by slower growth and diagnosis in the early stages, which improves the results of treatment for uterine cancer.
Type II (non-endometrioid cancer) – includes serous, clear cell, and other rare variants. Not associated with estrogen exposure, more commonly has a high degree of malignancy, aggressive course, and is found in later stages, making treatment of uterine cancer difficult [2].
Clinical Stage and Its Importance for Treatment
Staging is carried out according to the FIGO system and determines treatment tactics:
Stage ITumor is limited to the uterus; stage 1 uterine cancer treatment is usually represented by surgical options. In the presence of risk factors, adjuvant radiotherapy may be added. In most cases, it has high survival rates.
Stage IILesion extends to the stroma of the cervix, but does not extend beyond the organ; requires combined stage 2 uterine cancer treatment. Extended surgical treatment is performed with mandatory regional lymph node assessment. Postoperative radiotherapy or/with chemotherapy is often recommended.
Stage IIIProcess goes beyond the uterus with damage to adjacent tissues or lymph nodes; combined stage 3 uterine cancer treatment involves a combination of radical surgery and systemic therapy.
Stage IVDistant metastases (bladder, intestines, lungs) are present. Tactics are determined individually: possible cytoreductive intervention, systemic chemotherapy, targeted or immunotherapy, as well as palliative treatment. At this stage, treatment of uterine cancer aims to control the disease and improve the quality of life.
The stage of the disease determines the scope of therapy: in the early stages, the main method is surgery, while in advanced forms, radiation and/or chemotherapy are added to the treatment to improve oncological results [3].
Standard Treatment for Endometrial Cancer
The tactics of uterine cancer treatment are determined by the stage of the disease, which allows the elaboration of an individual, evidence-based treatment plan. In stage 0 uterine cancer treatment, when changes are limited to uterine lining, it is possible to use hormonal therapy or organ-preserving minimally invasive methods, especially in women who plan to maintain fertility.
For treatment for uterine cancer stage 1, in particular at stage 1A, the standard is surgery – total hysterectomy with bilateral salpingo-oophorectomy. This ensures radical removal of tumor within the uterus and accurate determination of the pathological stage. Today, laparoscopic and robotic techniques are increasingly used due to their safety, faster recovery, and positive impact on survival.
In stage II, where the tumor spreads to the cervix but remains within the organ, treatment includes extended surgery followed by adjuvant therapy (radiation and chemotherapy indicated) to reduce the risk of recurrence.
In the case of stage III, when the process goes beyond the uterus or affects the lymph nodes, uterine cancer treatment is usually combined: the operation with radiation and systemic chemotherapy. Radiation therapy controls local disease, while systemic treatment affects possible long-term spread. The decision is made individually at the tumor board meeting, taking into account the histology and general condition of the patient.
Understanding modern endometrial uterine cancer treatment options and following the recommendations allows you to choose the best treatment for uterine cancer according to the stage, minimizing side effects and optimizing clinical results [9, 10].
The tumor board decision described above — taking into account histology and the patient's general condition — depends on the completeness of the diagnostic record that arrives with the patient. For international patients, ER/PR receptor status, MMR/MSI characterization, and p53 mutation data are frequently absent. Type II cancers — serous, clear cell — carry different systemic therapy implications than endometrioid variants, and that distinction requires confirmed histological subtyping, not presumed staging.
Booking Health identifies which characterizations are present in the incoming record and arranges any missing profiling in Germany before the tumor board convenes.
Although laparoscopic surgery, radiation and chemotherapy remain basic components of uterine cancer treatment, modern oncology is actively implementing innovative approaches that increase the effectiveness and reduce the toxicity of therapy. Among them are – dendritic cell therapy and HIPEC, which show convincing results in a more targeted effect on the malignant process.
Interventional radiology is also developing rapidly, offering minimally invasive techniques. Together, these approaches form a new strategy of endometrial uterine cancer treatment, focused on personalization and improvement of clinical outcomes.
Dendritic Cell Therapy for Endometrial Cancer: Harnessing the Body’s Immune System
Dendritic cell therapy is a modern form of immunotherapy that activates the patient's own immune system. Dendritic cells recognize tumor antigens, present them to T-lymphocytes, and trigger a specific antitumor response. The discovery of the role of dendritic cells by Ralph M. Steinman was awarded the Nobel Prize in Physiology or Medicine in 2011 [4], which became the basis for the further development of this therapy.
Today, this method is considered a promising option for advanced endometrial cancer treatment, especially in cases of relapse or metastasis, when standard capabilities are limited. The approach involves isolating the patient's own dendritic cells, programming them with tumor-specific antigens, and re-administration to activate a targeted immune response.
Clinical data suggest improved tumor control and reduced toxicity compared to conventional chemotherapy. Thus, dendritic cell therapy expands the possibilities of womb cancer treatment, complementing standard approaches from stage 1a endometrial cancer treatment to the treatment of cancers that are advanced or diagnosed after menopause.
HIPEC for Endometrial Cancer: Targeted Chemotherapy Under Heat
This advanced endometrial cancer treatment is designed for cancers that have spread within the abdominal cavity, including advanced cases with metastasis. It combines surgical removal of all visible tumors with the delivery of heated chemotherapy directly into the abdomen.
HIPEC is a modern method of endometrial cancer treatment, which is used in the spread of the tumor process in the abdominal cavity, particularly in cases of metastasis. The method combines radical surgical removal of all visible foci of the malignant process with intra-abdominal administration of heated chemotherapy.
Hyperthermia (41-43°C) enhances the action of cytostatics [5]: heat increases the permeability of tumor cell membranes, improves drug penetration, disrupts repair mechanisms and increases cytotoxicity. Local delivery allows you to reach high concentrations of the drug without significant systemic load, which reduces side effects.
The procedure is performed immediately after surgery and aims to destroy microscopic tumor residues, which contributes to improved survival and reduced risk of recurrence in carefully selected patients. Thus, HIPEC expands the possibilities of treatment for endometrial cancer, especially in late stages in accordance with the principles of endometrial cancer treatment by stage.
Despite the need for careful selection of patients under the supervision of an experienced oncologist, this approach is increasingly integrated into modern treatment of endometrial cancer strategies, in particular in women with an intra-abdominal process.
"Careful selection of patients" is the clinical condition on which HIPEC's survival benefit depends. Peritoneal carcinomatosis index, performance status, and the absence of extra-abdominal disease are the variables selection criteria address — and they must be confirmed against current imaging before the procedure is proposed.
A patient who travels to Germany on the assumption that HIPEC is appropriate, only to have that assumption revisited on arrival, loses both time and the cytoreductive window that makes the procedure most effective.
Booking Health evaluates each patient's imaging against criteria before the trip is organized.
For a closer look at the practical aspects and results of the method, an interview with an expert dedicated to the modern application of HIPEC can be viewed.
VIDEO
Leading German Surgeon Dr. Lipp Reveals the Power of HIPEC in Cancer Treatment
General and Abdominal Surgery, Hepatopancreatobiliary Surgery and Hernia Surgery
Interventional Radiology in the Treatment of Uterine Cancer
Interventional radiology provides a modern, organ-sparing approach within complex oncology care in womb cancer treatment, particularly, in advanced, recurrent or inoperable cases. These minimally invasive procedures are performed under visual control and allow you to target the tumor, preserving healthy tissues as much as possible. This approach is especially important for patients who are contraindicated for surgery or need a combination of local and systemic therapy.
Several interventional methods for the treatment of uterine cancer and its metastasis are already successfully used in clinical practice.
Targeted Attack on Endometrial Tumors: How TACE and TACP Deliver Chemotherapy from Within
Transarterial chemoembolization (TACE) is a minimally invasive procedure increasingly integrated into modern endometrial uterine cancer treatment – especially for patients with pelvic or metastatic lesions resistant to systemic therapies. While it was initially developed for liver tumors, TACE has demonstrated promising results in gynecologic oncology, including cases of advanced or recurrent uterine cancer with metastasis to the pelvis, lymph nodes, or liver.
The TACE procedure involves two main stages. First, the interventional radiologist conducts a microcatheter through the femoral or radial artery to the vessel supplying blood to the cancerous focus. Next, a high concentration of the chemotherapy drug is injected directly into the tumor artery, after which embolization agents are used to block the blood flow. This allows the doctor to keep the drug in the affected area, increase the local cytotoxic effect, and deprive the tumor of oxygen and nutrients, which leads to its necrosis. In the field of oncologic gynecology, such approaches are seen as important uterine cancer treatment options, especially when radical hysterectomy is not possible.
Transarterial chemoperfusion (TACP) is a related but distinct method. Unlike TACE, it does not involve embolization: chemotherapy is administered in a high flow without blocking blood vessels. This ensures wider penetration of the drug into tumors with diffuse or infiltrative vascularization, which is often observed with advanced forms of carcinoma of the pelvic organs.
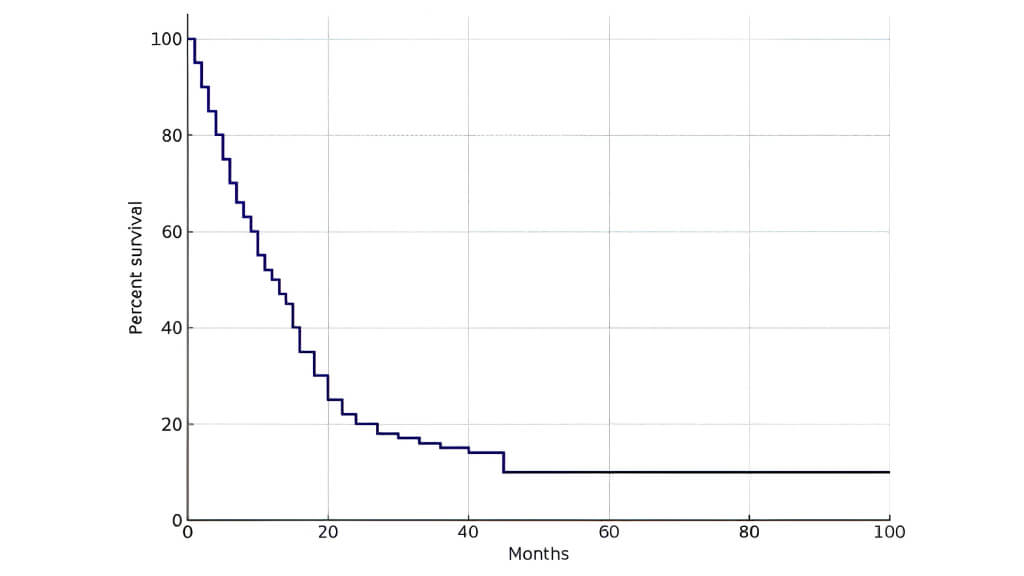
The latest data confirm the clinical effectiveness of both methods. Comparative analysis showed a statistically significant reduction in tumor size and favorable indicators of complete and partial response according to standardized assessment criteria. The median overall survival in the treated cohort was 16.15 months, highlighting the potential of these interventions in controlling advanced disease and related complications, particularly tumor bleeding. [6]
Quantitative assessment of changes in tumor size before and after transarterial chemoembolization and chemoperfusion
Therapy response and survival among patients with gynecologic tumors treated with transarterial chemoperfusion and transarterial chemoembolization [6]
Patient Group
Number of Patients
Median TV at Baseline (cm³)
3-Month Follow-Up
6-Month Follow-Up
9-Month Follow-Up
Group 1
46
117
98.48
-
-
Group 2
19
117.27
77.99
68.78
-
Group 3
10
103.4
86
80.87
119.71
Tumor response evaluation for different therapy protocols
Therapy response and survival among patients with gynecologic tumors treated with transarterial chemoperfusion and transarterial chemoembolization [6]
Tumor Response
TACP (n, %)
TACE (n, %)
TACP + TACE (n, %)
Stable disease
23 (70)
10 (50)
18 (82)
Partial response
6 (18)
3 (15)
-
Complete response
1 (3)
1 (5)
-
Progressive disease
3 (9)
6 (30)
4 (18)
Therapy responders
30 (91)
14 (70)
18 (82)
Curve of the overall survival of the entire patient cohort [6]
Radioablation (Radiofrequency Ablation) for Endometrial Cancer
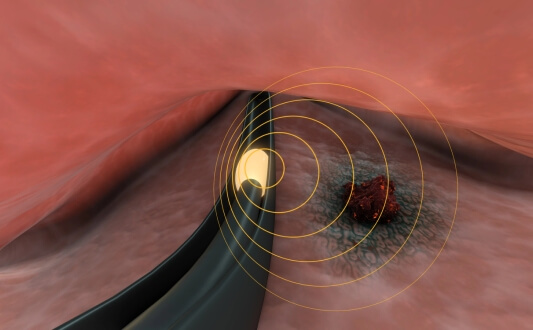
Radiofrequency ablation applies thermal energy to destroy tumor tissue: under imaging control, the needle electrode is injected directly into the tumor, and high-frequency current causes coagulation necrosis.
In the practice of oncologic gynecology, RFA is used for local relapses or metastasis in the pelvis, lymph nodes, lungs, or liver. The method is characterized by high accuracy, preservation of surrounding structures (including tissues near the uterine lining) and is valuable for patients who are contraindicated for repeated surgery or radiotherapy. The procedure is minimally traumatic, often outpatient, helps reduce tumor load, control pain and improve the quality of life within complex oncology care [7].
Cryoablation for Uterine Cancer
Cryoablation destroys tumor cells by extreme cooling. Under visual control, the probe is injected into the tumor, forming an "icy ball" that destroys cellular structures and blocks blood supply.
The method is effective in metastatic or recurrent forms of uterine cancer, particularly in soft tissues, lymph nodes and bones. It provides clear intraoperative visualization and the ability to accurately control the affected area. The procedure is usually performed under local anesthesia, characterized by rapid recovery and can be repeated as needed.
Thermoablation (Microwave Ablation) for Endometrial Cancer
Microwave ablation is a type of thermal ablation that uses electromagnetic energy to heat and destroy a tumor. Compared to RFA, MWA reaches higher temperatures and can be more efficient for larger foci.
As part of treatment of endometrial cancer, it is used for metastasis in the liver or lungs, as well as for pelvic relapses, when surgical intervention is impossible. The method provides reliable local control with minimal damage to healthy tissues and is often integrated into an individual treatment plan and multidisciplinary tumor board solutions, in particular with aggressive histological variants such as papillary subtypes [8].
RFA, cryoablation, and MWA are not interchangeable for the same metastatic lesion. Lesion size, location relative to vascular or biliary structures, and prior ablation history each point to different modalities — and the 70°C ablation zone achievable with MWA addresses different anatomical situations than cryoablation's ice ball expansion.
Booking Health maps each patient's metastatic pattern to the candidate center's specific ablation capabilities, identifying which institution has the documented procedural experience the lesion requires — not which center has the broadest general interventional radiology menu.
A Supportive Path Abroad: Suzanne’s Journey Through Advanced Uterine Cancer Treatment with Booking Health
When Suzanne Lynne O’Donoghue from the United Kingdom of Great Britain was diagnosed with advanced endometrial cancer, the search for treatment abroad was accompanied by uncertainty. After the confirmation of the diagnosis with a biopsy and other radiological examinations, she faced difficulties in organizing a medical trip. Contacting Booking Health helped structure the process and quickly gain access to Germany's leading clinic, which operates in accordance with modern endometrial cancer treatment guidelines and offers a wide range of uterine cancer treatment options.
The company organized her treatment in Frankfurt, providing professional support at all stages. From the first contact, Suzanne felt the support of the team, which took into account both the clinical aspects and the emotional state of the patient. All issues – from hospitalization to translation of medical documentation – were resolved continuously and in a coordinated manner.
Her personal coordinator, Afsaneh, played an important role in this experience. "She made the whole day smooth and helped us in everything so that the treatment was very easy and went well," noted Suzanne. Afsaneh provided a full understanding of each medical term, each stage of therapy, including issues relating to continued quality of life and preservation of fertility when appropriate.
Thanks to Booking Health's professional accompaniment, Suzanne was able to focus on the main – recovery. Her story demonstrates that reliable coordination can transform a complex treatment process abroad into a clearly organized and managed path to recovery. Regardless of the diagnosis, the right support makes access to highly specialized healthcare a real and vital decision.
Suzanne Lynne O’Donoghue and Professor Frank Gansauge
The Frankfurt clinic recommendation came before Afsaneh's coordination began. Booking Health's physician reviewed Suzanne's biopsy results, histological subtype, and prior treatment history before recommending that specific center — confirming it had the documented strengths in advanced endometrial cancer that her clinical situation required. The coordination Afsaneh provided was built on that clinical foundation.
The support felt seamless because the clinical decision had already been made correctly.
There Is a Way Forward – Even in Advanced Endometrial Cancer Cases
A diagnosis of advanced or recurrent uterine cancer often brings overwhelming emotions and difficult decisions. For patients facing late-stage disease, including those in need of stage 4 uterine cancer treatment, concerns about prognosis, potential recurrence, and limited treatment options can feel paralyzing. However, advanced does not mean untreatable.
Booking Health provides access to leading European oncology centers that specialize in the best treatment for uterine cancer, including rare and complex cases. Depending on the individual clinical picture, treatment may include surgery, chemotherapy, hormone therapy, immunotherapy, or innovative techniques such as interventional radiology – all combined in a personalized program designed to achieve the best possible outcome.
Each clinical case is analyzed individually, taking into account the patient's general condition, previous treatment, screening results, and tumor characteristics. Such a personalized approach is particularly important in the later stages, when standard protocols may not provide the desired effect.
Booking Health provides professional management of all stages of a medical trip – from the selection of a specialized clinic and medical team to the organization of medical documentation translation, and accommodation. This allows patients to focus on treatment without worrying about complex international logistics.
For women with advanced uterine cancer, Booking Health opens access to modern therapies and offers a clearly structured treatment route based on medical expertise and a patient-centered approach.
Best Hospitals For Endometrial Cancer Treatment in 2026
The choice of uterine cancer treatment centers is crucial in increasing survival rates and reducing the risk of recurrence. Today, leading clinics combine complex surgery, modern systemic therapy, and interventional methods (which allow them to offer personalized treatment protocols).
German endometrial cancer hospitals are especially popular among international patients. Multidisciplinary teams include: gynecological oncologists, chemotherapists, radiologists, and reproductive specialists. They provide a full range of services: from early diagnosis and robotic gynecological surgery to modern radiation therapy and molecular tumor profiling.
Best Hospital For Endometrial Cancer Treatment in 2026
Hospital
Country
Key Strengths
Why It’s Highly Rated
University Hospital LMU Munich
Germany
Robotic and minimally invasive surgery, fertility preservation
High-volume center with advanced surgical techniques and multidisciplinary care
Precision oncology, targeted therapies, and endocrine follow-up
University Hospital LMU Munich
LMU Munich is distinguished by its scientific activity and technological equipment – the clinic specializes in robotic gynecological surgeries (including minimally invasive hysterectomy). Multidisciplinary teams evaluate each case. Ovarian preservation and fertility programs are available for young patients. LMU Munich is virtually best cancer center for endometrial cancer in Europe.
University Hospital Ulm
The Ulm clinic is known for its expertise in the treatment of rare and aggressive forms of endometrial cancer (such as uterine sarcomas). Here, doctors perform radical operations with lymph node dissection and comprehensive systemic therapy (patients also can participate in research). Postoperative care includes not only relapse control but also psychological support and rehabilitation. Ulm is one of the best endometrial cancer hospitals in Germany.
Asklepios Hospital Barmbek Hamburg
Asklepios Barmbek specializes in early detection and minimally invasive surgery. Here, patients can undergo a hysterectomy with a gentle effect on the hormonal balance, as well as get quick access to diagnostics and postoperative therapy. The clinic meets the standards of the German Society of Oncology and is among the best hospital to treat endometrial cancer.
University Hospital Tuebingen
The University Hospital of Tübingen offers comprehensive treatment for endometrial cancer–including robotic surgery and radiotherapy. The center combines modern technologies with high clinical experience and provides access to international scientific studies and personalized care (guaranteeing patients safe and effective treatment).
Other world leaders in the treatment of uterine cancer (USA, UK, and others) also offer high-tech programs and a multidisciplinary approach, which allows achieving high results and maintaining the quality of life.
A Medical Journey: Every Step of the Way With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for already 12 years, Booking Health possesses solid expertise in creating complex cancer management programs in each individual case. As a reputable company, Booking Health offers personalized uterine cancer treatment plans with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment.
We provide:
Assessment and analysis of medical reports
Development of the medical care program
Selection of a suitable treatment location
Preparation of medical documents and forwarding to a suitable clinic
Preparatory consultations with clinicians for the development of medical care programs
Expert advice during the hospital stay
Follow-up care after the patient returns to their native country after completing the medical care program
Taking care of formalities as part of the preparation for the medical care program
Coordination and organization of the patient's stay in a foreign country
Assistance with visas and tickets
A personal coordinator and interpreter with 24/7 support
Transparent budgeting with no hidden costs
Health is an invaluable aspect of our lives. Delegating management of something so fragile yet precious should be done only to experts with proven experience and a reputation. Booking Health is a trustworthy partner who assists you on the way of pursuing stronger health and a better quality of life. Contact our medical consultant to learn more about the possibilities of personalized treatment with innovative methods for uterine cancer with leading specialists in this field.
Modern Cancer Treatment: Patient Journeys with Booking Health
Diane O. (United Kingdom), March 2026
Monica A. (Croatia), October 2025
Eliza A. (Armenia), June 2025
Susan Clark L. (USA), April 2025
FAQ: Understanding Uterine (Endometrial) Cancer and Its Treatment
What is the most effective treatment for uterine cancer?
Optimal tactics depend on the stage, the type of carcinoma and the general condition of the patient. In the early stages, the basis is surgery (often hysterectomy). Chemotherapy, radiotherapy or immunotherapy can be also added to the treatment plan.
How is uterine cancer diagnosed and staged?
In the practice of gynecology, the examination begins with complaints (for instance, abnormal bleeding) and imaging. Biopsy of the tissue of uterine lining confirms the presence of malignant cells. To determine the stage, additional examinations are performed to check for metastasis, after which the oncologist forms a treatment plan.
What are the different treatment options for uterine (endometrial) cancer?
Among the approaches are – laparoscopic or robotic surgery, radiotherapy, chemotherapy, hormone therapy and immunotherapy. The decision is made by a multidisciplinary tumor board, taking into account the type of tumor, damage to cervix or pelvic structures.
Is surgery always required for uterine cancer?
In most cases, hysterectomy is the standard option. However, with contraindications or in order to preserve fertility, hormone therapy or radiotherapy may be used.
What is a hysterectomy and how does it relate to uterine cancer?
This is the removal of the uterus, sometimes along with cervix and ovaries. It is often a first-line method in early endometrial carcinoma and can be performed laparoscopically or robotically.
Can uterine cancer be treated without removing the uterus?
Yes, in carefully selected early cases, hormone therapy is used under the strict supervision of an oncology care specialist, but the prognosis depends on the biology of the tumor.
What are the side effects of chemotherapy for uterine cancer?
Chemotherapy may cause fatigue, nausea, alopecia, cytopenia, and an increased risk of infections. It affects cancerous cells, including possible distant cells.
How does radiation therapy work for uterine cancer?
Radiotherapy destroys malignant tumor in the uterus, pelvic area, or lymph nodes. It can be external or internal (brachytherapy), depending on the stage.
What are the chances of recurrence after uterine cancer treatment?
The risk of recurrence is determined by stage, histology (for example, papillary subtypes), and primary treatment. Regular control improves prognosis and survival.
Is immunotherapy used for uterine (womb) cancer?
Yes, immunotherapy is used in advanced or recurrent forms with appropriate molecular markers and is part of modern oncology practice.
Can you still get pregnant after uterine cancer treatment?
With conservative hormonal treatment of early forms, pregnancy is sometimes possible. After a standard hysterectomy, natural fertility is lost.
Are there new treatments available for uterine (endometrial) cancer?
Innovative approaches include dendritic cell therapy, HIPEC, and TACE, aiming to reduce the risk of recurrence and improve survival rates.
What is the role of hormone therapy in uterine cancer treatment?
Hormone therapy affects hormone-sensitive tumor endometrial cells, slowing their growth, and may be part of an individual plan.
What is the cost of uterine cancer treatment?
The price depends on the country, the clinic, and the selected treatment plan. Booking Health helps organize effective treatment, second opinions, and offers full coordination.
What are the typical costs of endometrial (uterine) cancer treatment across countries, including Australia?
Estimated full-course costs: Germany – €80,000-150,000 (standard) /€25,000-60,000 (innovative); United Kingdom – €90,000-165,000 /€70,000-120,000; USA – €100,000-180,000 /€100,000-150,000. In Australia, access to innovative methods is limited and can be significantly more expensive than in Europe.
What is the 2-year survival rate for endometrial (uterine) cancer by treatment type?
The rates depend on the stage and type of carcinoma. Under the standard approach (surgery +/- chemotherapy +/- radiotherapy), a 2-year survival is 55-70% in the early stages and about 30% when the process is running with metastasis. Innovative methods (HIPEC, dendritic immunotherapy, interventional oncology) in individual cases demonstrate 60–75%.
What response rates are seen in endometrial (uterine) cancer treatments?
Standard therapy may give <10% response. Innovative approaches after the tumor board solution show approximately 45–65% in selected patients.
How long does treatment typically take for endometrial (uterine) cancer?
Classic schemes (chemotherapy, radiotherapy +/- surgery) last weeks or months. Innovative techniques are often completed in about 4 sessions with shorter recoveries.
What is the best treatment option for endometrial cancer?
The choice depends on the biology of the tumor and the stage. In Germany, the combination of immunotherapy, interventional radiology and HIPEC expands the possibilities of modern oncology care.
Which hospital is the best for endometrial cancer treatment?
The best hospitals for uterine cancer treatment work on a multidisciplinary principle and integrate complex methods within the framework of modern oncology.
What country is the best for endometrial cancer treatment?
Germany offers personalized treatment strategies for endometrial carcinoma that improve disease control and reduce the risk of recurrence.
Choose treatment abroad and you will for sure get the best results!
Authors:
This article was edited by medical experts, board-certified doctors Dr. Nadezhda Ivanisova, and Dr. Yana Dmytryshyn. For the treatment of the conditions referred to in the article, you must consult a doctor; the information in the article is not intended for self-medication!
Our editorial policy, which details our commitment to accuracy and transparency, is available here. Click this link to review our policies.
Sources:
01. Binhua Zhu, Hao Gu, Zhihan Mao et al. Global burden of gynaecological cancers in 2022 and projections to 2050. J Glob Health. 2024 Aug 16;14:04155. doi: 10.7189/jogh.14.04155.[DOI][PMC free article]
02. Jaclyn C Watkins, Michael J Downing, Marta Crous-Bou et al. Endometrial Tumor Classification by Histomorphology and Biomarkers in the Nurses' Health Study. J Cancer Epidemiol. 2021 Mar 12;2021:8884364. doi: 10.1155/2021/8884364.[DOI][PMC free article]
03. Stergios Kopatsaris, Ioannis Tsakiridis, Georgios Kapetanios et al. Management of Endometrial Cancer: A Comparative Review of Guidelines. Cancers (Basel). 2024 Oct 24;16(21):3582. doi: 10.3390/cancers16213582.[DOI][PMC free article]
04. Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x.[DOI][PubMed]
05. Iason Psilopatis, Christos Damaskos, Nikolaos Garmpis et al. The Role of Hyperthermic Intraperitoneal Chemotherapy in Uterine Cancer Therapy. Int. J. Mol. Sci.2023, 24(15), 12353; doi.org: 10.3390/ijms241512353.[DOI]
06. Thomas J. Vogl, Andreea I. Nica, Christian Booz et al. Therapy Response and Survival among Patients with Gynecologic Tumors Treated with Transarterial Chemoperfusion and Transarterial Chemoembolization. Medicina 2024, 60(10), 1585. doi:10.3390/medicina60101585.[DOI]
07. Robert L Dood, Clarisa R Gracia, Mary D Sammel et al. Endometrial cancer after endometrial ablation versus medical management of abnormal uterine bleeding. J Minim Invasive Gynecol. 2014 Feb 28;21(5):744–752. doi: 10.1016/j.jmig.2014.02.012.[DOI][PMC free article]
08. Chris Brace. Thermal Tumor Ablation in Clinical Use. IEEE Pulse. 2011 Sep-Oct;2(5):28–38. doi: 10.1109/MPUL.2011.942603.[DOI][PMC free article]
09. Theresa M Kuhn, Saeeda Dhanani, Sarfraz Ahmad. An Overview of Endometrial Cancer with Novel Therapeutic Strategies. Curr Oncol. 2023 Aug 27;30(9):7904–7919. doi: 10.3390/curroncol30090574.[DOI][PMC free article]
10. Stefano Restaino, Chiara Paglietti, Martina Arcieri et al. Management of Patients Diagnosed with Endometrial Cancer: Comparison of Guidelines. Cancers (Basel). 2023 Feb 8;15(4):1091. doi: 10.3390/cancers15041091.[DOI][PMC free article]
thank you for reaching out! One of our medical advisors is currently reviewing your details. You can expect a call from us within one business day to discuss your request.
Note: The incoming call will appear as a German number or your local area code. This call is entirely free of charge.
Booking Health guarantees:
Expert Placement
We use rigorous statistical analysis to ensure you are treated at the best-rated facility for your specific diagnosis.
Total Cost Protection
No hidden fees or unexpected bills. We provide a fixed price guarantee, backed by insurance that covers any additional complications.
12-Month Extended Care
Your recovery is our priority. Benefit from a full year of direct medical support following your procedure.