
Colorectal cancer claims more than 930,000 lives in a single year [3], and the distance between a stage I and stage IV diagnosis is not a medical abstraction. It is the difference between a disease that surgery resolves and one that requires a fundamentally different strategy to manage. Over 1.9 million new cases were recorded globally in 2020 [2], making it the third most prevalent cancer in the world and the second leading cause of cancer-related death [1]. The disease concentrates in individuals over 50, not arbitrarily, but because the transformation from benign polyp to invasive malignancy is a process measured in years — years during which screening can intervene.
Where the cancer is found within that progression determines what treatment can realistically offer. Colorectal cancer treatment by stage dictates not just which tools are available, but what those tools can reasonably be expected to achieve — which is why staging is not a bureaucratic classification but a clinical decision with direct consequences for the patient's path forward. The 5-year relative survival rates make that consequence visible: approximately 91% for stage I, 85% for stage II, 73% for stage III, and 13% for stage IV [4, 5].
Those numbers are not a verdict. Immunotherapy, targeted therapy, and personalized treatment planning in the colorectal cancer treatment guideline are changing outcomes at every stage — including stage IV, where patients once out of options are now pursuing remission and rebuilding lives they had been told to wind down.
Standard Treatment Protocols for Colorectal Cancer
Because colorectal cancer presents so differently depending on when it is found, no single protocol applies across its full range — stage, tumor location, and the patient's overall condition determine which interventions are viable and in what sequence [6]. Surgery addresses what is localized and physically removable. Stage I disease may require only polypectomy or local excision; tumors that have grown through the intestinal wall demand segmental resection — colectomy or proctectomy — removing the affected bowel segment alongside regional lymph nodes to give patients in stages I through III their strongest chance at complete remission.
Adjuvant chemotherapy in stage III is not to be used or not: it targets the microscopic residual disease that surgery has no instrument to remove. Clinical evidence shows that chemo reduces recurrence risk to the level that resection alone cannot achieve. The goal changes to "control" (slowing progression, symptoms management) in patients with metastatic disease.
Radiation acts most precisely on rectal cancer. Preoperative delivery shrinks the tumor before surgery and reduces local recurrence risk in the pelvic region. For disease that has progressed beyond curative intent, it manages what surgery and systemic therapy cannot reach — the bleeding, obstruction, and localized pain that advanced colorectal cancer produces in tissue it has already claimed.
New and Innovative Colorectal Cancer Treatment Options
Dendritic Cell Therapy for Colorectal Cancer
When conventional treatment stops working, the problem is rarely the drug itself — it is that the tumor has restructured its biology specifically to survive it. Dendritic cell therapy enters where that resistance begins, not by overpowering the cancer with a stronger agent, but by enlisting the one system the tumor cannot fully predict: the patient's own immune response. Dendritic cells are antigen-presenting cells that teach T-cells to identify and act against specific threats; harvested from the patient, exposed to tumor-specific antigens in a laboratory, and reintroduced into the body, they activate an immune response directed precisely at the malignancy. In dendritic cell therapy for colon cancer, the attack that follows is not pharmacological. It is biological — built from the patient's own immune architecture, trained to recognize what it previously missed, and now pursuing the cancer on terms the tumor did not anticipate.
The Nobel Prize in Physiology or Medicine was awarded in 2011 to Ralph Steinman for his discovery of dendritic cells and their key role in initiating the immune response [7]. It shows that the method is scientifically recognised, and this laid the groundwork for developing dendritic cell-based immunotherapies.
Research has shown the great results of dendritic cell-based vaccines even in 4 stage bowel cancer treatment. It indicated that combining dendritic cell therapy with standard chemotherapy even more facilitates immune activation in colorectal cancer patients and contributes to tumor regression. That’s why, to improve overall survival rates and quality of life for patients with metastatic colorectal cancer, the combination of therapies is used.
The combination of DC vaccination with chemotherapy is not additive by default — it depends on timing. Chemotherapy administered immediately before vaccination can suppress the immune cell population the vaccine needs to activate; administered at the right interval after, it can enhance antigen release and prime a stronger T-cell response.
Booking Health's case review confirms whether the proposed combination protocol at the candidate colorectal cancer treatment center reflects the sequencing conditions under which published efficacy data was generated — because the same two therapies in the wrong order can produce a meaningfully different outcome.
CHECK IF A BETTER SOLUTION EXISTS FOR YOUHyperthermic Intraperitoneal Chemotherapy (HIPEC) for Colorectal Cancer
HIPEC is a new colorectal cancer treatment procedure that combines open cytoreductive surgery (CRS) with further administration of heated chemotherapy into the abdominal cavity. This treatment is used mainly for patients with metastatic peritoneal cancer. The procedure starts with the surgical removal of visible tumors. Then, the circulation of warmed chemotherapeutic agents is performed within the peritoneal cavity. The heat allows for better penetration of the chemotherapy and, by that, increases its effectiveness. Thanks to the procedure, the microscopic cancer cells that are left after the surgery are being destroyed.
Research indicated that CRS combined with HIPEC can significantly improve survival rates. A systematic review reported a 5-year survival rate increasing from 19% to 51% for patients who received this combined treatment.
If you seek a more in-depth understanding of HIPEC, we advise you to watch a video interview with Professor Michael Lipp, Head of Abdominal and Colorectal Surgery at Asklepios Hospital Barmbek. He dives into this process step-by-step and tells more about patient selection criteria and how HIPEC significantly improves outcomes for individuals with abdominal carcinomatosis.
VIDEO
Dr. Michael Lipp:
"The Future of Complex Cancer Surgery"
General and Abdominal Surgery, Hepatopancreatobiliary Surgery and Hernia Surgery
BOOK CONSULTATION
The 5-year survival improvement from 19% to 51% applies to patients who were correctly selected for CRS-HIPEC — those with limited peritoneal disease burden, adequate performance status, and no distant extra-abdominal metastases.
Patients who arrive without a prior eligibility assessment risk discovering that their peritoneal carcinomatosis index or surgical history excludes them from the procedure that motivated the trip.
Booking Health conducts that eligibility assessment against Dr. Lipp's published selection criteria before travel is organized.
GET A SECOND OPINION FOR YOUR CASEPressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for Colorectal Cancer
PIPAC is a minimally invasive alternative treatment for colorectal cancer. It is designed for patients with end-stage disease with peritoneal carcinomatosis from colorectal cancer. PIPAC improves standard chemotherapy by delivering drugs in the form of aerosol directly into the peritoneal cavity during laparoscopic surgery. This ensures uniform distribution and helps to penetrate the tissue more deeply. It is also designed for patients who are not appropriate candidates for a large surgical procedure. It is shown that PIPAC is a safe treatment that improves median overall survival, ranging from 8 to 37.8 months. Also, it keeps the patient’s quality of life stable between PIPAC cycles.
Interventional Radiology for Colorectal Cancer
Interventional radiology (IR) has now become a consistent component in the management of patients with colorectal cancer with advanced-stage disease and those who are not candidates for traditional surgery. It is a set of image-guided, minimally invasive procedures and targeted treatments that can effectively control tumor growth but also minimize damage to surrounding healthy tissues.
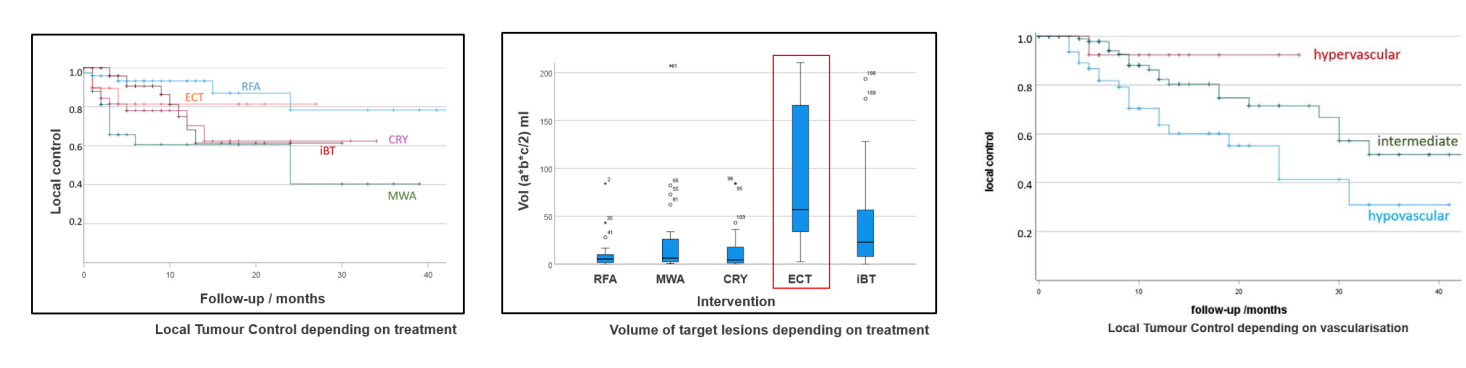
Thermal ablation is one of the main IR techniques, which includes radiofrequency ablation (RFA) and microwave ablation (MWA). These methods are aimed at destroying the tumor by delivering heat directly to the lesion. This helps to effectively "cook" the malignant tissue at the same time preserving surrounding healthy structures as much as possible. Thermal ablation can achieve local control rates of 80-90% and 5-year overall survival rates exceeding 50% in patients with liver metastases. These techniques are often performed under image guidance (CT or ultrasound) and can be repeated if new lesions appear. They are typically used for tumors less than 3 cm in size and are ideal for patients who are not candidates for surgery due to other health conditions.
Cryoablation is a technique that, with the help of extreme cold, causes the tumor cell apoptosis through ice crystal formation and cellular rupture. It is a particularly great method for tumors located near critical blood vessels or nerves, because it allows for precise control with minimal damage to surrounding tissues. Cryoablation also works with real-time visualization that increases precision. In patients with colorectal cancer, it is used for both curative and palliative purposes. In some cases, it can also stimulate a local immune response against the tumor.
VIDEO
Prof. Kovács on Electrochemotherapy:
How Electric Pulses Help Chemo Actually Work
Interventional Radiology
BOOK CONSULTATION
The reason chemotherapy sometimes fails is not always pharmacological — it is structural: the drug cannot enter the cancer cell in concentrations high enough to destroy it. Electrochemotherapy addresses that problem at the membrane level. Brief electrical pulses temporarily increase cell membrane permeability and allow chemo-agents to penetrate tumor cells far more efficiently than standard systemic delivery permits — which is why cytotoxic effect increases while overall drug exposure to healthy tissue decreases. Clinical studies in patients with colorectal cancer liver metastases have demonstrated objective response rates of up to 85.7% and a median progression-free survival of approximately 9 months. For patients with limited remaining treatment options, those figures are not incremental. ECT is minimally invasive, well-tolerated, and applicable to cutaneous, subcutaneous, and internal lesions including those in the liver and pelvic region — which means patients who have already exhausted standard protocols can still be pursuing active, evidence-based best treatment for colorectal cancer.
Stent placement is an IR technique that can be used when the tumor blocks the bowel and causes obstruction. The procedure is image-guided and starts with the placement inside the narrowed part of the rectum the self-expanding metal stent to restore stool passage. It is an important new treatment of colorectal cancer for patients who can’t undergo surgery due to serious comorbidities. It is a palliative treatment for improving the quality of life by reducing symptoms such as pain, bloating, and constipation. Stent placements are performed under local anesthesia due to their minimal invasiveness and have a quick recovery time. This makes it perfect for patients with advanced colon cancer who are not candidates for immediate surgery.
Transarterial chemoembolization (TACE) is an IR technique that targets cancer and metastases by delivering chemotherapy directly to the blood vessels supplying the tumor with further obstruction. This minimizes the systemic side effects and targets cancer more effectively. TACE is one of the main options for patients with liver metastases, especially in stages III and IV, where surgical options may not be that effective. In this case, chemotherapy is administered through a catheter into the hepatic artery feeding the tumor. The embolization provides the blockage of the artery and traps the chemotherapy inside. This approach reportedly has an increased disease control rate of up to 54.3% and a median survival of 47.4 months in patients treated with TACE.
The interventional radiology techniques described above — thermal ablation, cryoablation, ECT, TACE — are not interchangeable. Tumor size, proximity to hepatic vasculature, prior radiation exposure, and whether the target lesion is primary or metastatic each determine which technique is appropriate.
Booking Health maps each patient's imaging against the specific procedural capabilities of the candidate best colorectal cancer treatment centers, because a center that performs TACE but not ECT will recommend what it can do rather than what the tumor's characteristics indicate. The clinical question and the institutional menu are only the same when the right colorectal cancer center has already been identified.
FIND THE RIGHT SPECIALIST FOR YOUR CASEAdvantages of Interventional Radiology for Colorectal Cancer
With each improvement in oncology procedures, IR plays a great role in new colorectal cancer treatment, especially for patients with complex or advanced disease. Compared to the traditional surgical procedures, it is minimally invasive. Thanks to that, it has several advantages, including reduced surgical trauma, shorter hospital stays, and faster recovery. Techniques like ablation, chemoembolization, and stent placement are now becoming standard procedures for colorectal cancer treatment, including early interventions in colorectal cancer stage 1 treatment and more aggressive strategies for stage 3 colorectal cancer treatment or even at 4 stage colorectal cancer treatment. These treatments are aimed at sparing as much healthy surrounding tissue as possible, minimizing side effects, and making them highly targeted.
Also, minimally invasive procedures like thermal ablation and laparoscopy-guided therapies can be repeated by an oncologist, which is essential in the cases of advanced and aggressive cancers. IR is a great option for rectal cancer treatment, 4 stage rectal cancer, and rare cases like small bowel cancer treatment or duodenal cancer treatment. It offers a modern solution to problems that conventional methods may not have been able to solve. Also, the combination of IR and systemic therapies, like immunotherapy for bowel cancer, gives patients a chance for much-improved outcomes. The IR use is usually put into the treatment plan by multidisciplinary teams. For a lot of patients, these procedures successfully support long-term remission, transforming standards of oncological care.
FAPI PET Imaging and FAPI-Based Therapy for Colorectal Cancer
When liver metastases determine the entire treatment strategy, an incomplete lesion count doesn't just blur the picture — it can point toward the wrong procedure entirely. FAPI PET for colorectal cancer changes what's visible by targeting fibroblast activation protein in the tissue surrounding tumor cells, rather than relying on glucose metabolism the way standard PET-CT does. In the liver specifically, this matters because healthy tissue is metabolically active enough to hide small metastatic deposits on FDG imaging.
That clarity feeds directly into decisions about TACE, thermal ablation, and surgical candidacy. FAPI PET for colorectal cancer metastases can confirm the true extent of hepatic involvement before a procedure is planned — and the gap between three visible lesions and five isn't a rounding error. It's the difference between ablation alone, TACE, or a combined approach. The same logic extends to the peritoneum, where FAPI's low background uptake in the abdomen can resolve findings that CT leaves ambiguous, informing the HIPEC or PIPAC eligibility discussion that follows.
What FAPI PET doesn't provide is an automatic bridge to treatment. FAPI therapy for colorectal cancer — pairing the targeting molecule with a therapeutic radionuclide such as Lutetium-177 — remains investigational, and FAP expression varies considerably between tumors, and even between metastatic sites within the same patient. The scan comes first for a reason: it establishes whether this pathway has biological relevance before any therapeutic decision gets made.
Booking Health's case review includes FAPI PET assessment where it may add value, connects patients with German centers offering the scan, and provides cost clarity within the broader treatment plan.
Comparison Between Colorectal Cancer Treatments Abroad
* Booking Health data
| Colorectal cancer treatment types | 2-Year Survival Rate | Response Rate | Duration | Side Effects |
|---|---|---|---|---|
| Colorectal Cancer Standard Treatments | ~25% for advanced cancer | Less than 10% | Several cycles | Severe (nausea, fatigue, hair loss, immunosuppression, skin irritation) |
| Colorectal Cancer Latest Treatment | ~60% for advanced cancer | 45-65% | Up to 4 sessions | Mild (localized discomfort) |
Medical Procedures Costs Around the World for Colorectal Cancer
* Prices may vary depending on the course of treatment and tumor characteristics
| Treatment Method | GERMANY* | GB | USA |
|---|---|---|---|
| Standard Treatment | €80,000 - €150,000 full course | €90,000 - €165,000 full course | €100,000 - €180,000 full course |
| Innovative Methods | €25,000 - €60,000 full course | €70,000 - €120,000 full course | €100,000 - €150,000 full course |
Patients coordinating through Booking Health access treatment options for colorectal cancer in Germany pricing without the foreign patient surcharge that a colorectal cancer treatment clinic routinely applies to self-referred international inquiries — a surcharge not reflected in published ranges. The savings on a full innovative course can reach €30,000–€60,000 compared to equivalent UK pricing alone.
A fully itemized budget is provided before any commitment is made, and complication insurance covering up to €200,000 is included as standard.
Get full treatment coordination supportReal Colorectal Cancer Patient Story: Success with TACE
Colorectal cancer treatment is a complex thing to deal with, especially in the advanced stages. Let’s look at the case of Sarasibala Premachandran from the United Kingdom, who found hope even when battling a serious disease. She was diagnosed with stage 4 colon cancer and chose to travel to Germany with the help of Booking Health. She had a consultation and went with a treatment plan from Professor Thomas Vogl, one of the leading experts in interventional oncology at the University Hospital in Frankfurt. Sarasibala underwent a TACE procedure, a targeted and minimally invasive interventional radiology procedure directly to liver tumors with further blood supply blockage.
What struck Sughandi, Sarasibala’s daughter, first was not the medicine or the best hospital for colorectal cancer — it was the consistency. From the first day her mother entered treatment, Booking Health provided the kind of logistical and emotional scaffolding that allows a family in crisis to stop managing details and focus on the person they came to help. Procedures were explained before they happened, communication between doctors and family was facilitated rather than left to chance, and the Premachandran family was never made to feel like outsiders navigating a system that wasn't built for them.
Sarasibala's prognosis today is hopeful — not because the system was kind to her, but because the clinical match was precise. Her liver metastasis pattern and disease burden pointed specifically toward interventional radiology as the primary modality. Which is why she was directed to Prof. Vogl: his documented outcomes in TACE for colorectal liver metastases made him the right physician for her disease, not for her case in the abstract. The empathy Sughandi experienced was real. The clinical reasoning that made it possible came first.
Advanced Cancer Treatment: Patient Success Stories with Booking Health













Treating Late-Stage Colorectal Cancer: A Personalized Approach
A stage 4 colorectal cancer diagnosis does not arrive as information — it arrives as a sentence, and most patients absorb it that way. The words "there is little that can be done" close a door that oncology, in many cases, has already found another way through. TACE, HIPEC, and dendritic cell therapy are not consolation options for patients who have exhausted everything else — they are interventions designed for the specific biological conditions that advanced disease creates, targeting tumor characteristics that standard protocols were never built to address. Because they act locally or through the patient's own immune system rather than systemically, they produce fewer side effects, shorter stays at a colorectal cancer treatment hospital, and more time at home — which is not a secondary benefit. For patients with metastatic disease, it is often the condition that makes continued treatment sustainable.
Booking Health matches patients to the best colorectal cancer hospitals in Germany and specialists whose documented outcomes align with their specific disease profile — not to the nearest available oncology unit.
That matching is the work that happens before a colorectal cancer new treatment begins, and it is what determines whether the treatment chosen has a realistic chance of working for the disease in front of it.
In the most advanced stages, the option that changes everything is often the one a patient finds only because someone helped them look in the right place — and finding it is where recovery begins.
Even in the most advanced stages, there can be an option that will work just for you. With modern therapies becoming more available, patients who undergo a 4 stage colorectal cancer treatment have meaningful and active lives.
A Medical Journey: Every Step of the Way with Booking Health
Finding the most effective treatment of colorectal cancer can be challenging, especially for patients already fatigued by multiple therapies, conflicting opinions, and complicated medical terminology. With so many standard treatment protocols offering limited success and often accompanied by harsh side effects, patients are frequently left unsure of how to move forward.
This is where Booking Health steps in. As a trusted international medical facilitator with over 12 years of experience in oncology coordination, we help patients worldwide gain access to innovative therapies at the best European hospitals. Our strength lies in building personalized cancer treatment strategies based on each patient's diagnosis, clinical data, and prognosis, ensuring not only advanced care but a path toward better recovery and improved survival rates.
Booking Health provides full-service coordination, including:
- Medical report assessment and expert consultation
- Development of a tailored medical care program
- Selection of a suitable hospital for colorectal cancer treatment
- Preparation and translation of documents
- Communication with treating physicians
- Visa support, flight, and accommodation arrangements
- A personal coordinator and interpreter available 24/7
- Support before, during, and after treatment, including follow-up care in your home country
- Transparent pricing with no hidden costs
Your health is too important to entrust to chance. With Booking Health, you are supported by a professional team dedicated to ensuring the most effective care available, designed around you.
Booking Health holds ISO 9001 quality certification, reflecting well-established processes and strict quality control at every stage of the treatment journey — not just at the initial consultation, but throughout.

Frequently Asked Questions About Colorectal Cancer
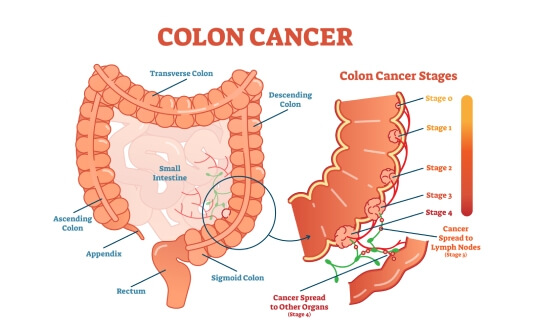
Colorectal cancer takes its name from the two structures it arises in — the colon and the rectum, which together form the large intestine's final passage. Because the colon spans several anatomically distinct segments — ascending, transverse, descending, and sigmoid — the disease can develop at different points along this tract, each with implications for how it is staged, accessed surgically, and treated.
Roughly 150,000 Americans receive a colorectal cancer diagnosis each year, making it the fourth most common cancer in the country. A lifetime risk of approximately 1 in 24 for men and 1 in 26 for women means this is not a disease that requires unusual circumstances — it is common enough that the decision not to screen carries real consequences.
Early detection makes colorectal cancer curable in a significant proportion of patients — and even stage 3 disease, and selected stage 4 cases, can achieve long-term remission when advanced treatment combinations are applied. The boundary between curable and manageable shifts depending on when the disease is found, which is precisely why that timing matters so much.
Colonoscopy with biopsy gives clinicians direct visualization of the intestinal lining and tissue confirmation of malignancy. CT and MRI imaging then define how far the disease has extended beyond the bowel wall, while blood tests — including CEA tumor marker levels — establish a baseline for tracking treatment response and detecting recurrence once therapy ends.
Carcinoembryonic antigen — CEA — is the marker clinicians rely on most to evaluate treatment response and monitor for recurrence in colorectal cancer. A single CEA value tells only part of the story; what matters clinically is the direction it moves — falling during treatment signals response, rising after treatment ends signals the need for immediate investigation.
Colorectal cancer typically develops over several years, beginning as polyps that form in the intestinal lining long before they become malignant. That slow progression is not reassuring in itself — it is only meaningful if it is used: regular screening during this window is what converts a gradual biological process into a preventable disease.
Stage 3 colorectal cancer is approached with curative intent in many patients, and the evidence supports that ambition. Surgery followed by chemotherapy significantly reduces the risk of recurrence and improves survival — which means a stage 3 diagnosis, serious as it is, does not determine the outcome. The treatment plan that follows it does.
The answer depends entirely on the patient's specific disease — its stage, anatomical location, genetic mutations, and individual factors that shift what each therapy can realistically achieve. Surgery, chemotherapy, targeted therapy, radiation, and immunotherapy are each effective within the conditions that call for them; the clinical skill lies in assembling the combination that fits the disease in front of the clinician, not the disease described in a protocol.
Surgical resection, chemotherapy, radiation therapy, targeted agents, and immunotherapy form the core of colorectal cancer treatment — with radiation applied most specifically to rectal cancer, where local control before or after surgery changes long-term outcomes. Advanced-stage disease that has spread to distant sites may also be addressed through localized interventional techniques such as HIPEC and TACE, which act on metastatic deposits through mechanisms systemic therapy cannot replicate.
Surgery is the most frequently used intervention, particularly across stages I through III where the disease remains localized and complete resection is achievable. Chemotherapy follows in most cases — not because it is routine, but because microscopic residual disease that surgery cannot physically remove requires a systemic response to prevent it from establishing a recurrence.
In stage 3 disease, chemotherapy after surgery meaningfully reduces recurrence risk — which is not a statistical abstraction but a clinical decision that changes how many patients remain disease-free five years later. In metastatic disease, it extends survival and preserves quality of life, particularly when molecular profiling guides which agents are selected rather than defaulting to a standard regimen regardless of the tumor's biology.
Surgery is recommended when the cancer is localized and technically resectable — when a complete removal is achievable without leaving disease at the margins. In carefully selected advanced cases where metastases are limited in number and location, surgery may still be part of the plan, but that decision rests on whether the patient's overall disease biology supports an operative approach or whether systemic control needs to come first.
Fatigue, nausea, diarrhea, neuropathy, and reduced immune function are common during active treatment — each shaped by the specific agents used and how the patient's body responds to them. Long-term effects, including bowel dysfunction and surgical complications, can persist after therapy ends. Addressing these is not separate from treating the cancer; a patient who cannot tolerate the full course of therapy because side effects are unmanaged is a patient whose treatment has been compromised before it is complete.
Targeted therapy acts on the specific molecular vulnerabilities that a tumor's genetic mutations create — RAS, BRAF, and HER2 alterations each make cancer cells dependent on pathways that corresponding drugs are designed to block. In advanced colorectal cancer, targeted agents are typically combined with chemotherapy, extending the reach of systemic treatment into biological territory that chemotherapy alone cannot address and that surgery has no access to.
Dendritic cell vaccination trains the immune system to recognize and act against tumor cells by presenting them with the specific molecular signals needed for identification — a mechanism that works from within the patient's own biology rather than through external pharmacological pressure. Results have been most encouraging when this approach is combined with conventional therapies, suggesting that an immune response activated by dendritic cell vaccination is most effective when the tumor's defenses are simultaneously disrupted by other means.
Radiation therapy is applied primarily to rectal cancer, where the anatomy allows precise targeting and where shrinking the tumor before surgery — or reducing recurrence risk after it — changes outcomes in measurable ways. Colon cancer is treated with radiation far less frequently, because the colon's mobility within the abdominal cavity makes consistent targeting difficult and systemic therapy covers most of the same clinical ground.
Five-year relative survival rates track closely with stage at diagnosis: approximately 91% for stage I, 85% for stage II, 73% for stage III, and around 13% for stage IV. That progression is not inevitable — it is the consequence of detection timing. Each stage boundary crossed before diagnosis is a survival percentage that screening could have protected.
Recurrence is most likely within the first three to five years after treatment ends, which is why structured follow-up during that window is not optional. Blood tests, imaging, and clinical review at regular intervals are the mechanism that catches returning disease while it is still localized enough to treat — because recurrence found early remains a clinical problem; recurrence found late becomes a different one entirely.
Treatment costs range from approximately $25,000 for stage 1 colorectal cancer treatment to over $150,000 when advanced disease requires multiple therapies or complex interventional procedures. Stage and treatment intensity are the primary cost drivers — which means the most accurate estimate for any individual patient begins with a review of their specific diagnosis, not a general price range.
Metastatic colorectal cancer is increasingly addressed through immunotherapy, combination targeted therapies, and localized interventional techniques — HIPEC, PIPAC, and TACE — each designed to act on disease that has spread beyond the reach of surgery and standard chemotherapy. For patients whose cancer has stopped responding to first-line treatment, these are not experimental footnotes. They are the interventions most likely to change what the disease can still do.
Best colorectal cancer treatment options 2026 include dendritic cell immunotherapy, HIPEC, and TACE. They are helping patients to achieve 45-65% response rates compared to less than 10% with standard treatments. It is a new hope for advanced cases.
Oncological teams have significantly improved late colorectal cancer survival rates through modern treatments such as TACE and PIPAC. These minimally invasive approaches have ~60% 2-year survival rates compared to ~25% with conventional protocols.
Colon vs rectal cancer treatment differences, whether or not it is appropriate to have radiation therapy. Rectal cancer often requires preoperative radiation. It helps to shrink tumors, while colon cancer relies mainly on surgery and chemotherapy.
Yes, in some cases, it is possible to treat cancer without surgery. The alternatives are thermal ablation, cryoablation, electrochemotherapy, and TACE. These are minimally invasive techniques that can provide effective tumor control even for a late stage colorectal cancer.
The cost of colon cancer treatment in Europe vs. the USA is really different. Germany offers patients innovative treatments for €25,000-€60,000 versus €1000,000-€150,000 in the USA. Affordable colorectal cancer treatment abroad also adds to excellent patient care, psychological support, and rehabilitation.
Symptoms of colorectal cancer can be nonspecific and include changes in bowel habits, blood in the stool, abdominal discomfort, unexplained weight loss, and fatigue. However, in the early stages, the disease may show no signs, showing the importance of screening.
The 2-year survival rate for advanced colorectal cancer can reach 25% if the patient is treated with standard options. But, with innovative approaches such as HIPEC, TACE, or dendritic cell therapy, survival rates may increase to around 60%.
Standard colorectal cancer treatment involves multiple chemotherapy cycles that can take several months or a few years. On the other hand, innovative therapies like PIPAC, HIPEC, dendritic cell therapy, etc., usually require only one or up to four sessions.
People who are receiving standard therapies for colorectal cancer often report nausea, fatigue, hair loss, and immunosuppression. In comparison, innovative treatments tend to have milder, localized side effects, which significantly improve tolerance.
The response rate to standard chemotherapy for colorectal cancer is typically below 10%. In turn, innovative multimodal therapies achieve response rates of 45-65%, particularly when interventional, immune, and targeted methods are combined.
Colorectal cancer treatment requires a balance between controlling the primary tumor and managing metastases. In Germany, patients can access dendritic cell therapy, HIPEC, PIPAC, interventional radiology, and hyperthermia ㄧ these approaches allow precise targeting of tumors (often achieving results beyond what standard chemotherapy can provide).
Leading hospitals for colorectal cancer focus on combining surgical expertise with cutting-edge therapies. German oncology centers offer advanced treatment options ㄧ enabling individualized plans that adapt to tumor location, stage, and patient response.
Germany is considered one of the best countries for colorectal cancer care due to its availability of advanced interventions. You can have access to dendritic cell therapy, HIPEC, PIPAC, interventional radiology, and hyperthermia, which allows patients to receive personalised treatments.
Choose treatment abroad and you will for sure get the best results!
Sources:
01. World Health Organization, WHO. Colorectal cancer. https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer
02. OncoDaily. Colorectal Cancer: Epidemiology, Pathogenesis, Diagnosis, and Therapeutic Advances. https://oncodaily.com/oncolibrary/cancer-types/colorectal-cancer
03. Eileen Morgan, Melina Arnold, A Gini et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023 Feb;72(2):338-344. doi: 10.1136/gutjnl-2022-327736. Epub 2022 Sep 8. [DOI] [PubMed]
04. American Cancer Society. https://www.cancer.org/
05. Prashanth Rawla, Tagore Sunkara, Adam Barsouk. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019 Jan 6;14(2):89–103. doi: 10.5114/pg.2018.81072. [DOI] [PMC free article]
06. Cancer Research UK. Treatment options for colon cancer. https://www.cancerresearchuk.org/about-cancer/bowel-cancer/treatment/treatment-colon/treatment-decisions
07. Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x. [DOI] [PubMed]
Read:
01. New Effective Treatments for Stage 4 Cancer: Innovations in Oncology