
Prostate cancer (PCa) stands as the second most common cancer diagnosis among men worldwide. Each year brings approximately 299,000 new cases in the United States alone—representing 14.9% of all new cancer diagnoses [1]. The five-year survival rate for localized PCa approaches 100%, while patients with regional disease maintain survival rates above 99% [1]. These remarkable outcomes stem from decades of technological advancement and refined treatment protocols.
Current data shows a 15-year relative survival rate of 97% across all stages [1]. What makes this even more encouraging? Advanced radiation techniques continue to push these numbers higher while simultaneously reducing treatment of prostate cancer burdens and side effects.
What Is Radiation Therapy Treatment and How It Works in Prostate Cancer Treatment
Radiation therapy (RT) is a treatment method for cancer, which involves the use of ionizing radiation. RT destroys prostate cancer cells through high-energy particles that damage cellular DNA. Unlike surgery, which physically removes the prostate gland, radiation precisely targets malignant tissue while preserving surrounding structures [2]. And according to modern scientific concepts, radiation therapy for prostate cancer is comparable in the effectiveness to the radical prostatectomy.
The following types of traditional radiation therapy for prostate cancer are available:
- As the main treatment method for localized PCa (T1-T2 stages), if surgical treatment is contraindicated for the patient
- As the main treatment method for more advanced prostate cancer, when the surgery for removal of gland will not give the desired result and androgen deprivation therapy (ADT) is not indicated
- RT is performed in addition to surgical treatment after prostatectomy in order to destroy the remaining prostate cancer cells and prevent a recurrence
When radiation beams penetrate prostate cancer cells, they create breaks in the DNA double helix—the blueprint that allows cells to divide and multiply. Healthy cells possess robust repair mechanisms. How does it kill cancer cells? They lack these sophisticated defenses [3]. Consequently, malignant cells die while normal tissue recovers. Over weeks of treatment, this differential effect accumulates, systematically eliminating the tumor.
Modern radiation oncology has evolved far beyond simple beam delivery. For instance, image-guided techniques (IGRT) – CT scanning, magnetic resonance imaging – now allow physicians to track the tumor's position in real-time and adjust for natural movement caused by bladder filling or rectal changes [4]. Other treatments difference: traditional external beam therapy typically spans 4-6 weeks with daily sessions. Newer hypofractionated radiation therapy regimens compress this to 2-3 weeks by delivering higher doses per session [5]. And much more. We will take a closer look at each technique further.
Types of Radiation Therapy Used to Treat Prostate Cancer
Radiation oncology offers multiple pathways to cure. The field has progressed from one-size-fits-all approaches to personalized medicine, where treatment selection considers tumor characteristics and personal priorities.
External Beam Radiation Therapy (EBRT)
External beam radiation therapy (EBRT) involves external radiation exposure of the pelvic area. During the external radiation therapy, the patient lies on a special table, a linear accelerator moves around him and directs ionizing beams. The full course of standard radiation therapy for prostate cancer lasts 6-7 weeks. About 5 RT sessions are carried out per week.
The main stages of external beam radiation therapy for prostate cancer:
- Planning (simulation) of radiotherapy. At this stage, the required position of the patient's body and special immobilizing devices for fixation of the body are selected. After that, a computed tomography of the pelvis is performed, the localization and spreading of the prostate tumor are determined. Special marks are made on the patient's skin in order to indicate the target irradiation zone. It may also be necessary to place metal markers in the prostate.
- Elaboration of a radiation plan. With the help of images obtained, radiologists use a computer program to delineate the tumor. Then they create the RT plan – the doctors determine from which sides and at what angles it is better to irradiate the tumor, as well as calculate radiation dose.
- Radiotherapy session. On the appointed day, the patient comes to the clinic for the first session. He is asked to lie down on the linear accelerator table. CT scan is carried out to make sure that the patient is in the correct position. The accuracy of the irradiation depends on this. After all preparations, the session is started.
Intensity-Modulated Radiation Therapy
Thanks to the use of modern equipment, RT has become more accurate and safer. In leading foreign hospitals, irradiation is carried out on linear accelerators, operating in the IMRT mode.
Multiple beams of varying intensities approach from different angles, each modulated to "paint" radiation onto the tumor while minimizing healthy tissue exposure [6]. Clinical trials demonstrated that IMRT reduced both gastrointestinal and genitourinary toxicity compared to 3D-CRT while maintaining equivalent cancer control. One landmark study reported only 12% of patients experienced significant bowel symptoms at 15 months with IMRT, versus 21% without this advanced technique [7].
Higher dose escalation improves outcomes. The GETUG-AFU 18 trial provided level 1 evidence: men with high-risk prostate cancer who received 80 Gy versus 70 Gy experienced 77% overall survival at 10 years compared to 65.9%, with progression-free survival improving from 72.2% to 83.6% [8]. Importantly, higher doses caused no additional long-term toxicity when delivered with modern techniques.
Contact Radiation Therapy – Brachytherapy Treatment
Internal radiation therapy is called brachytherapy (BT). The essence of this treatment method is the insertion of radioactive granules inside the entire prostate gland. Thus, targeted irradiation of the prostate tumor occurs. Due to the short radius of radiation exposure, adjacent healthy tissues are not damaged by radiation. Brachytherapy is called the most sparing treatment for prostate cancer (early-stage).
There are two options for brachytherapy to treat prostate cancer:
- Low dose-rate brachytherapy (LDR). This treatment method involves a single insertion of radioactive material into the prostate. The implanted granules emit radiation for 1-3 months, and after the irradiation completion there is no need to remove them from the patient's body.
- High dose-rate brachytherapy (HDR). During this type of treatment, catheters are inserted into the prostate, through which radioactive granules with a high dose of radiation are administered. The catheters are removed 15 minutes after the course completion. The procedure is carried out 2-3 times.
Certain clinics do specialize in this method, e.g. University Hospital of Ludwig Maximilian University of Munich and Helios Hospital Berlin-Buch. These specialized centers perform hundreds of brachytherapy procedures annually, with excellent results.
Proton Therapy for Prostate Cancer
Proton therapy (PT) achieves what conventional radiation cannot: a dose distribution that stops at the tumor's back edge. Unlike high-energy rays, X-rays, which pass through the body delivering exit doses beyond the target, protons deposit maximum energy at a specific depth—the Bragg peak—then halt abruptly [9].
This physical advantage translates to dosimetric superiority. Proton beams spare the rectal wall and peripheral tissues more effectively than even advanced photon techniques. Simulation studies estimated proton therapy could reduce second cancer risk by 26-39% compared to IMRT [9]—a meaningful consideration for younger men with decades of life expectancy.
But do these dosimetric benefits yield clinical advantages? The PARTIQoL trial provided definitive answers [10]. It enrolled 450 patients with low- or intermediate-risk localized prostate cancer, comparing proton beam therapy to IMRT. After median follow-up exceeding 5 years, researchers found no differences in quality of life (QoL) at any timepoint. Bowel function scores remained essentially identical. Cancer control matched expectations—both techniques achieved excellent biochemical control rates!

Stereotactic Body Radiation Therapy (SBRT) for Prostate Cancer
Five sessions. Not five weeks—five sessions total, delivered over 1-2 weeks. SBRT revolutionized convenience in cancer care by compressing entire courses into ultra-precise, high-dose sessions.
The concept challenges traditional radiobiology. Conventional approach tells that spreading radiation over many small doses allowed normal tissue recovery between procedures. SBRT delivers 7-9 Gy per fraction instead of the traditional 2 Gy. Emerging evidence suggests PCa may actually respond more favorably to these larger doses per fraction due to its unique radiobiological properties [6].
Toxicity patterns differ. SBRT patients initially report more genitourinary / gastrointestinal symptoms (GU / GI)—peak in first 2 years. However, these differences resolve by 5 years. Bowel function remains comparable throughout. The transient urinary symptoms can be managed effectively with medications.
Not every patient qualifies as an ideal SBRT candidate. Men with large prostate glands, pre-existing significant urinary symptoms, or inflammatory bowel conditions may fare better with conventional fractionation. Ongoing trials will define SBRT's role beyond low- and intermediate-risk disease.
Dr. med. Peter Stoll, director of the Radiation Oncology Clinic Pasing in Munich and recognized as one of Munich's leading radiation oncologists by FOCUS magazine. You can watch interview about advanced radiation techniques to professor’s practice.
Brachytherapy vs Radiation Therapy for Prostate Cancer
Brachytherapy is radiotherapy delivered from inside the body rather than externally – it is interstitial radiation therapy. This distinction matters because the two approaches offer complementary advantages for different clinical scenarios.
- External beam radiation excels at treating larger volumes. When cancer has extended beyond the prostate capsule or when pelvic lymph nodes require intervention, external beams can encompass these areas comprehensively. The convenience of outpatient treatment—arriving for daily sessions, leaving immediately afterward—appeals to many men.
- The method called low dose rate brachytherapy (LDR-BT) implants tiny radioactive seeds permanently into the prostate under ultrasound guidance. These rice-sized capsules emit radiation continuously for several months, delivering extremely high doses to the prostate while sparing surrounding organs. The steep dose gradient protects the nearby healthy tissue of rectum and bladder.
- High dose rate brachytherapy (HDR-BT) takes a different approach. Catheters placed into the prostate guide a highly radioactive source through each catheter for several minutes per session. After 2-4 procedures over 1-2 days, doctors remove the catheters. HDR brachytherapy allows even more precise dose sculpting than LDR.
Which approach proves superior? The answer depends on individual circumstances. For low-risk cancer confined to the gland, LDR brachytherapy alone achieves cure rates exceeding 95% at 10 years. Intermediate-risk disease often requires brachytherapy combined with external beam radiation for optimal outcomes.
Radiation Therapy vs Surgery in Prostate Cancer Treatment
The choice between radiotherapy and radical prostatectomy ranks among the most consequential decisions that men with early-stage cancer face. Both approaches offer curative potential; neither demonstrates clear superiority for cancer control in randomized trials [2]. The decision is often individual.
The landmark ProtecT trial provides rigorous comparison. This UK study randomized 1,643 men aged 50-69 with localized prostate cancer to active monitoring, surgery, or radiotherapy [2]. After 15 years of follow-up, 97% remained alive regardless of group. Cancer-specific mortality showed no significant differences. Both radical treatments halved the risk of metastasis and disease progression compared to monitoring.
Side effect profiles diverge substantially. Surgery carries immediate risks: urinary incontinence affects 10-20% of men at one year. Erectile dysfunction (ED) impacts 30-70% depending on age and surgical approach. Radiation therapy typically preserves erectile function better initially, though late effects accumulate over years.
Urinary side effects follow different patterns. Post-surgical incontinence tends to improve progressively over 12-24 months. Radiotherapy rarely causes incontinence but frequently triggers irritative urinary symptoms—frequency, urgency, nocturia—during and shortly after it. These typically resolve within 6 months.
The radiation therapy versus surgery debate ultimately lacks a universally correct answer. Both represent excellent options when performed expertly. Younger men with long life expectancy may prefer surgery's definitive removal of the cancer, accepting higher initial side effect risks. Men with comorbidities making anesthesia risky favor radiation's non-invasive approach.
Benefits of Radiation Therapy for Prostate Cancer Patients
Radiation therapy offers distinct advantages; understanding these benefits helps patients make informed decisions.
Non-invasive – avoids surgical risks entirely. No incisions, no anesthesia complications, no blood loss, no hospital recovery. For men with cardiac disease, diabetes, or other conditions increasing surgical risk, radiation's safety profile proves invaluable.
Excellent cancer control matches surgical outcomes. The method achieves biochemical disease-free survival rates equivalent to radical prostatectomy across all risk groups [2]. The 10-year metastasis-free survival reaches 96% for low-risk, 92% for intermediate-risk, and 80% for high-risk disease when treated with modern dose-escalated RT. These figures rival or exceed published surgical series.
Preservation of continence stands as most significant functional advantage. While 10-20% of surgical patients experience persistent urinary leakage requiring pads [2], stress incontinence after radiation therapy remains exceedingly rare—affecting less than 2% of patients even with long-term follow-up [6].
Flexibility accommodates individual anatomy and disease characteristics. For men with large prostatic glands exceeding 80-100 grams, radiation avoids the technical challenges such size creates for surgical removal.
Technological advances continue improving outcomes. Techniques like SBRT reduce treatment time dramatically. Rectal spacers placed near rectum before radiation reduce rectal dose and toxicity [7]. And so on.
| Characteristics/Therapy type | 2-Year Survival Rate | Response Rate | Duration | Side Effects |
|---|---|---|---|---|
| Standard Treatment | ~25% for more advanced cancers | Less than 10% | Several cycles | Severe (nausea, fatigue, hair loss, immunosuppression, skin irritation) |
| Innovative Methods | ~60% for more advanced cancers | 45-65% | Up to 4 sessions | Mild (localized discomfort) |
View Prostate Cancer Care Guide
Where Is the Best Place for Radiation Therapy?
Various clinics differ significantly in terms of technical equipment. Unfortunately, many clinics still have to work with outdated one due to insufficient financing. In this case, the likelihood of post-radiation complications is high.
At the same time, the doctors from leading foreign hospitals use modern medical equipment, which is updated regularly. This allows them to achieve the best therapeutic results with minimal risk of side effects. The following countries are the best for RT in urological cancer:
- Germany
- USA
- Great Britain
- Australia
Germany is the leader in the treatment of cancers. Following the link, you can find information about the most popular hospitals for prostate cancer radiation therapy in Germany.
| Germany | €28,000 - €42,000 |
| Great Britain | €35,000 - €65,000 |
| USA | €40,000 - €80,000 |
| Australia | €21,000 - €37,000 |
Why Choose Radiation Therapy for Prostate Cancer in Germany?
Germany is a premier destination for international patients who seek advanced radiation therapy for prostate cancer – and here is why.
Advanced equipment: in addition to widespread options, IMRT, IGRT, VMAT and SBRT are available here. The concentration of proton centers in Germany exceeds most other European countries.
Specialization reaches impressive depths. Large university hospitals operate dedicated cancer centers certified by the German Cancer Society. Physicians at these centers treat cancer in hundreds or thousands of cases annually—a volume that breeds expertise impossible to achieve in lower-volume settings.
Quality assurance standards. German medical facilities undergo rigorous certification processes. Cancer centers must document outcomes, complication rates, and patient satisfaction scorest. Equipment undergoes regular calibration and verification testing – to maintain accuracy.
Multidisciplinary team (MDT) work – here, tumor boards unite urologists, radiation oncologists, medical oncologists, pathologists and any other healthcare professionals a patient may need.
Innovation access. For instance, Lu-177 PSMA for metastatic cancer was available in Germany years before widespread adoption elsewhere. Trials of novel treatment combinations, adaptive radiation treatment plans, and artificial intelligence-guided interventions proceed at German university hospitals.
Success rates exceeding 90% for localized disease, achieved with minimal long-term complications – this is what thousands of international patients look for annually.
Here you see the video interview where Dr. Birte Schneevoigt – a specialist in urology and andrology at the Urology Clinic Wiener Platz in Munich – shares her insights on modern prostate cancer treatments, such as RT and innovative approaches.
Patient Experience and Outcomes of Prostate Cancer Treatment Abroad
Michael Petersen faced the diagnosis when PSA screening revealed intermediate-risk PCa. After contacting and discussing options with different healthcare specialists, Michael chose radiation therapy at a German university hospital—a decision that proved transformative. "The precision of their IMRT planning impressed me, as I’m an engineer myself. The attending physician gave me confidence. I was sure that I was receiving the most advanced treatment available, exactly what I need" he recalls.
Throughout his treatment course, 62-year-old Michael experienced minimal side effects, continuing to work remotely between appointments. Eighteen months post-treatment, his PSA remains undetectable at 0.1 ng/mL – and he maintains normal urinary and sexual function.
A Medical Journey: Every Step of the Way With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for already 12 years, Booking Health possesses solid expertise in creating complex cancer management programs in each case. As a reputable company, Booking Health offers personalized prostate cancer treatment plans with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment. We provide:
- Assessment and analysis of medical reports
- Development of the medical care program
- Selection of a suitable treatment location
- Preparation of medical documents and forwarding to a suitable clinic
- Preparatory consultations with clinicians for the development of medical care programs
- Expert advice during the hospital stay
- Follow-up care after the patient returns to their native country after completing the medical care program
- Taking care of formalities as part of the preparation for the medical care program
- Coordination and organization of the patient's stay in a foreign country
- Assistance with visas and tickets.
- A personal coordinator and interpreter with 24/7 support
- Transparent budgeting with no hidden costs
Health is an invaluable aspect of our lives. Delegating management of something so fragile yet precious should be done only to experts with proven experience and a reputation. Booking Health is a trustworthy partner who assists you on the way of pursuing stronger health and a better quality of life. Contact our medical consultant to learn more about the possibilities of personalized treatment with innovative methods for metastatic prostate cancer with leading specialists in this field.
International Cancer Care: Patient Stories with Booking Health








FAQ About Radiation Therapy for Prostate Cancer
Send request for treatment15-year relative survival rate reaches 97% across all stages with radiation therapy for prostate cancer. Low-risk disease is up to 96% metastasis-free survival at 10 years, while intermediate-risk maintains 92%. And even high-risk cases achieve 80% with modern dose-escalated techniques.
Urinary symptoms after prostate radiation treatment typically emerge during course – frequency, urgency, nocturia – though most resolve within 6 months. Bowel side effects prostate radiation causes can include irritation and changes in bowel habits. Erectile dysfunction after radiation treatment develops gradually, over years – unlike immediate impact of surgery.
Life expectancy mirrors surgical outcomes. The ProtecT trial demonstrated 97% of men remained alive after 15 years regardless of treatment choice. Prostate cancer risk groups influence outcomes as well.
Side effects of radiation therapy for prostate cancer vary by technique. SBRT initially causes more genitourinary symptoms – peaking in the first 2 years before resolving. And traditional approaches trigger irritative urinary issues: urgency and frequency.
Current data shows exceptional outcomes. It is up to 97% overall survival at 15 years after prostate cancer radiation treatment. And what about prostate cancer-specific mortality? It is minimal across all approaches.
High-energy particles damage cancer cell DNA – that's the essence. Prostate cancer treatment options include external beams or internal radiation therapy. Cancer cells lack repair mechanisms that healthy tissue possesses and that leads to tumor elimination.
In selected men with localized prostate cancer radiation can be a first-line option offered by healthcare provider. Cardiac disease, diabetes, or conditions making anesthesia risky? Radiation offers safety without surgical complications. Large prostates exceeding 80-100 grams also benefit. Man seeking continence preservation – he is also candidate for radiation therapy for prostate cancer.
Brachytherapy types of radiation therapy for prostate cancer – these deliver radioactive sources directly. EBRT prostate cancer treatment that spans conventional approaches to advanced IMRT prostate cancer techniques. SBRT prostate cancer treatment that reduces course to just 5 sessions. Proton therapy prostate cancer irradiation – precisely stopping at the tumor's edge.
Irritative urinary symptoms typical for early treatment include frequency, urgency, nighttime urination – most resolve within months. Sexual function is preserved initially better than surgery, though late effects can accumulate. Bowel changes occur less frequently. Combined treatment for prostate cancer may intensify side effects, although temporarily.
Neither demonstrates superiority. The ProtecT trial proved radical prostatectomy vs radiation therapy achieve equivalent cancer control – 97% survival at 15 years regardless of choice. Radiation vs surgery prostate cancer care differs primarily in side effects. Surgery risks immediate incontinence, radiation – preserves continence but triggers irritative symptoms, etc.
Absolutely. Hormone therapy plus radiation for prostate cancer – the combination improves outcomes, in high-risk disease especially. The GETUG-AFU 18 trial demonstrated that ADT with radiation therapy for prostate cancer delivering 80 Gy achieved 77% overall survival versus 65.9% with lower doses. And advanced cases particularly benefit from this approach.
Choose treatment abroad, and you will for sure get the best results!
Authors:
This article was edited by medical experts, board-certified doctors Dr. Nadezhda Ivanisova, and Dr. Bohdan Mykhalniuk. For the treatment of the conditions referred to in the article, you must consult a doctor; the information in the article is not intended for self-medication!
Our editorial policy, which details our commitment to accuracy and transparency, is available here. Click this link to review our policies.
Source:
[1] Tyler B. Kratzer, Natalia Mazzitelli, Jessica Star et al. Prostate cancer statistics, 2025. CA Cancer J Clin. 2025;75(6):485-497. doi:10.3322/caac.70028. [DOI]
[2] Hamdy FC, Donovan JL, Lane JA, Metcalfe C, Davis M, Turner EL, et al. Fifteen-year outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2023;388(17):1547-1558. doi:10.1056/NEJMoa2214122. [DOI]
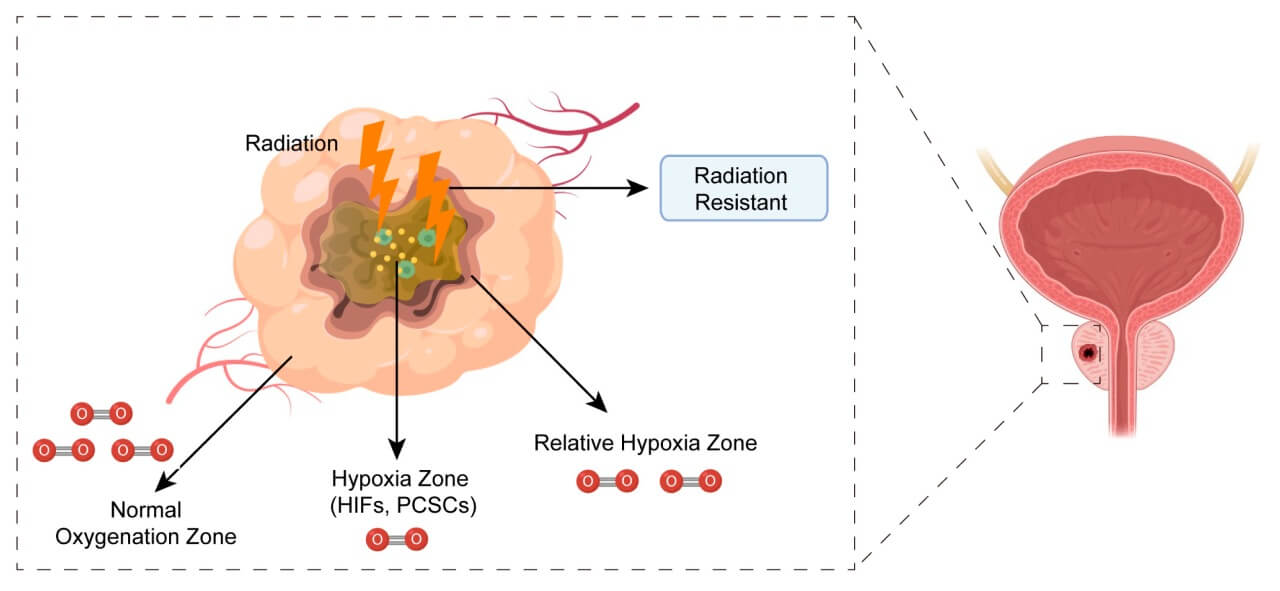
[3] Lyu F, Shang SY, Gao XS, Ma MW, Xie M, Ren XY, et al. Uncovering the Secrets of Prostate Cancer's Radiotherapy Resistance: Advances in Mechanism Research. Biomedicines. 2023;11(6):1628. doi:10.3390/biomedicines11061628. [DOI]
[4] Dang A, Kupelian PA, Cao M, Agazaryan N, Kishan AU. Image-guided radiotherapy for prostate cancer. Transl Androl Urol. 2018;7(3):308-320. doi:10.21037/tau.2017.12.37. [DOI]
[5] Dearnaley D, Syndikus I, Mossop H, Khoo V, Birtle A, Bloomfield D, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016;17(8):1047-1060. doi:10.1016/S1470-2045(16)30102-4. [DOI]
[6] Fischer-Valuck BW, Rao YJ, Michalski JM. Intensity-modulated radiotherapy for prostate cancer. Transl Androl Urol. 2018;7(3):297-307. doi:10.21037/tau.2017.12.16. [DOI]
[7] Hamstra DA, Mariados N, Sylvester J, Shah D, Karsh L, Hudes R, et al. Continued benefit to rectal separation for prostate radiation therapy: final results of a phase III trial. Int J Radiat Oncol Biol Phys. 2017;97(5):976-985. doi:10.1016/j.ijrobp.2016.12.024. [DOI]
[8] Hennequin C, Sargos P, Roca L, et al. Long-term results of dose escalation (80 vs 70 Gy) combined with long-term androgen deprivation in high-risk prostate cancers: GETUG-AFU 18 randomized trial. J Clin Oncol. 2024;42(4_suppl):LBA259. doi:10.1200/JCO.2024.42.4_suppl.LBA259. [DOI]
[9] Paganetti H, Beltran C, Both S, Dong L, Flanz J, Furutani K, et al. Roadmap: proton therapy physics and biology. Phys Med Biol. 2021;66(5):05RM01. doi:10.1088/1361-6560/abcd16. [DOI]
[10] Efstathiou JA, Yeap BY, Michalski JM, et al. Prostate Advanced Radiation Technologies Investigating Quality of Life (PARTIQoL): Phase III Randomized Clinical Trial of Proton Therapy vs. IMRT for Localized Prostate Cancer. Int J Radiat Oncol Biol Phys. 2024;120(2 Suppl):S1. doi:10.1016/j.ijrobp.2024.08.012. [DOI]
Read:
Comprehensive Guide to Prostate Cancer Treatment: New and Standard Treatment Options
Lutetium 177-PSMA: a new generation drug for prostate cancer treatment