
Neuroendocrine tumors have shown a significant increase in prevalence over the past two decades. Between 2000 and 2018, the age-standardized incidence increased from 4.9 to 8.2 cases per 100,000 population, with the most pronounced increase being among grade 1 tumors, early stages, and appendix neoplasms [1]. Despite improved diagnostic methods and better detectability, mortality among patients with neuroendocrine tumors has more than tripled during this time, which remains a serious clinical challenge.
Understanding Neuroendocrine Tumors
Modern capabilities of personalized medicine allow to significantly improve the results of treatment of patients with neuroendocrine tumors. NETs often require a multidisciplinary approach that combines advanced diagnostics, therapy, and long-term disease control strategies. Although neuroendocrine tumors (NETs) are relatively rare compared to other cancers, their complexity makes them a distinct and challenging group of diseases. They can behave very differently depending on where they originate, how aggressive they are, and how early they’re detected. Understanding the basic features of these cancers is crucial for proper diagnosis and treatment.
Understanding How NETs Develop
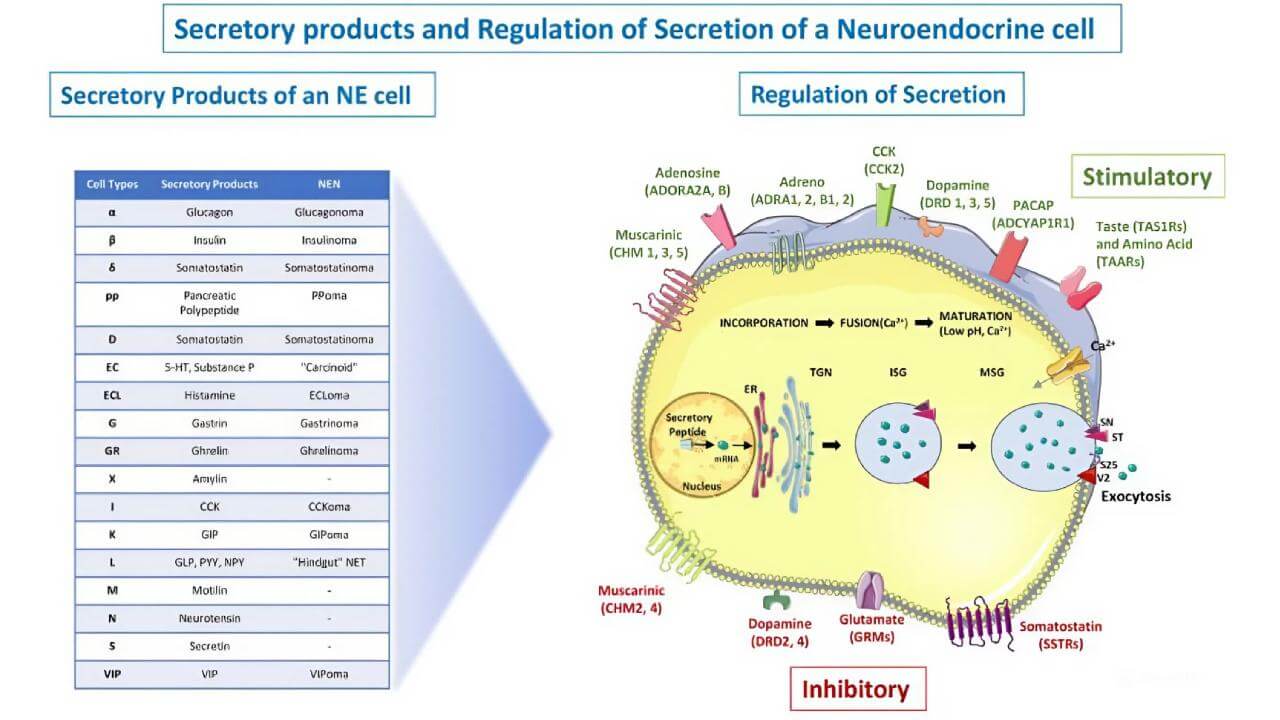
Neuroendocrine tumors arise from cells that have traits of both nerve and hormone-producing cells. These cells are scattered throughout the body, which is why NETs can occur in a variety of organs. What makes them unique is their ability to release hormones or hormone-like substances, sometimes causing distinct clinical syndromes.
Common Causes and Risk Factors of Neuroendocrine Tumors
In most cases, the exact cause of NETs is unknown. However, available information suggests that certain genetic conditions, such as multiple endocrine neoplasia type 1 (MEN1), can increase the risk. Other potential factors include chronic inflammation in the digestive tract, smoking (especially for lung NETs), and a family history of similar tumors. Still, many people develop NETs without any clear risk factors.
Symptoms of Neuroendocrine Tumors That Should Not Be Ignored
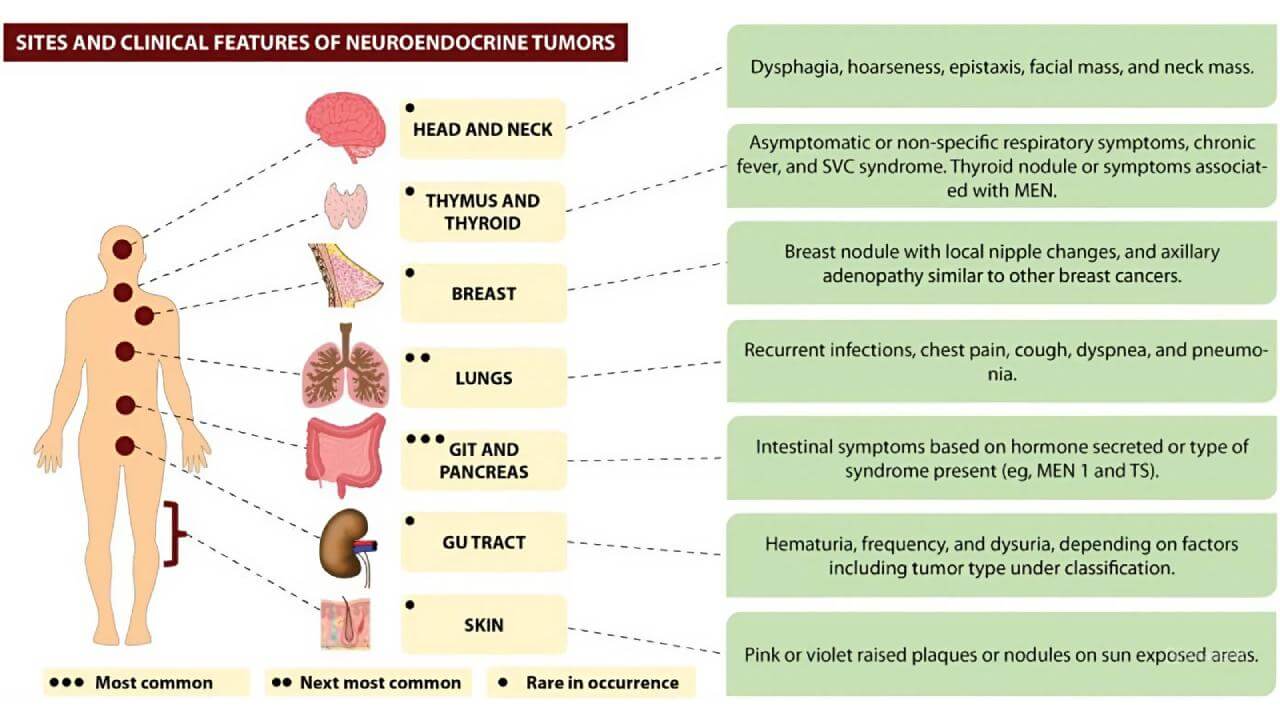
Clinical manifestations of neuroendocrine tumors vary depending on their location and hormonal activity. Some neoplasms can remain asymptomatic for a long time, while others cause pronounced signs already in the early stages.
Common symptoms include: abdominal pain, bowel dysfunction, flushing, wheezing, unexplained weight loss, and chronic fatigue. Hormonally active tumors can cause carcinoid syndrome with diarrhea, skin hyperemia, and valvular heart disease.
If such manifestations appear, it is important to contact clinical specialists in a timely manner at a specialized hospital, where a full-fledged examination can be carried out, and the appropriate therapy can be selected.
How NETs Are Classified
Neuroendocrine cancers are classified based on two main things: how much the tumor cells look like normal cells (this is called differentiation) and how quickly they’re dividing. Both factors help doctors understand how aggressive the tumor might be and choose the right treatment strategy.
The World Health Organization (WHO) divides NETs into three grades, depending on how fast the cells are growing [3].
This is measured by two markers:
- The mitotic rate – how many cells are dividing under the microscope
- The Ki‑67 index – a lab test that shows how many cells are in the active phase of growth
Here's a simplified breakdown:
- Grade 1 (G1): These are slow-growing tumors. Under the microscope, fewer than 2 cells per 10 high-power fields are dividing, and the Ki‑67 is below 3%.
- Grade 2 (G2): These tumors are more active, with 2 to 20 dividing cells and a Ki‑67 between 3% and 20%.
- Grade 3 (G3): These are fast-growing and potentially more aggressive tumors, with over 20 mitoses and Ki‑67 above 20%.
Most G1 and G2 tumors are called well-differentiated NETs and tend to grow more slowly. G3 tumors are usually poorly differentiated and referred to as neuroendocrine carcinomas (NECs) – a more aggressive form.
Diagnosis of Neuroendocrine Tumors
The examination of patients with neuroendocrine tumors is based on a combination of laboratory tests and modern imaging. Since such tumors can grow slowly and manifest atypically, several methods are used simultaneously to detect, assess activity, and select treatment options early. In specialized centers in Germany, diagnostic algorithms are comprehensive and meet modern cancer treatment standards.
Laboratory Tests and Tumor Markers
The examination usually begins with general blood tests with assessment of liver and kidney function, as neuroendocrine tumors can affect these organs.
Among the specific markers, the following are most often determined:
- Chromogranin A (CgA) – is the most common marker of the neuroendocrine tumor
- NSE – may increase with varying degrees of tumor differentiation
- Pancreatic polypeptide, gastrin, serotonin and its metabolite 5-HIAA – depending on the type of tumor
Although these markers are not absolutely specific, they are important for monitoring the course of the disease in patients and evaluating the response to therapy [10].
Hormonal Testing
In patients with neuroendocrine tumors that secrete hormones, determining their level is a key. Depending on the clinical picture, these can be evaluated:
- Serotonin and 5-HIAA (in carcinoid syndrome)
- Insulin, gastrin, VIP, somatostatin – in case of damage to the pancreas
- ACTH or cortisol – when adrenal glands are involved
These tests help identify functionally active tumors and adjust treatment.
Visualization: CT, MRI, PET-CT
Imaging techniques are crucial for diagnosis and staging [4].
- CT with contrast – is a basic method for determining the size and spread of the process
- MRI – is particularly informative in liver metastases and pancreatic tumors
- PET-CT – is a highly sensitive method for detecting somatostatin-receptor-positive formations; in many cases it is considered as a standard
- PET-CT with FDH is used in more aggressive forms
The combination of these approaches allows doctors to form a complete picture of the disease.
Biopsy and Morphological Confirmation
The final diagnosis is made after the biopsy. Pathology confirms the neuroendocrine nature of the tumor, determines its degree and the Ki-67 index, which reflects the growth rate.
These data are fundamental for choosing the optimal treatment tactics in a specialized clinic and predicting the course of the disease in patients with neuroendocrine tumors.
Ki-67 index, somatostatin receptor status, and CgA level are the three data points that most directly determine which treatment pathway — PRRT, DC vaccination, TACE, or systemic chemotherapy — is appropriate for a specific NET patient. These characterizations are frequently incomplete in records arriving from international patients, particularly those diagnosed in systems where NET-specific profiling is not routine.
Booking Health identifies which tests are absent from the incoming record and arranges the missing workup in Germany before the multidisciplinary team convenes, because a treatment plan built on incomplete tumor biology is not individualized care — it is an approximation.
FIND THE RIGHT SPECIALIST FOR MY CASEStandard Treatment Options for Neuroendocrine Tumors
Neuroendocrine tumors are characterized by significant biological diversity, so the approach to treatment is determined by their localization, degree of differentiation, stage and hormonal activity. Within the German healthcare system, protocols in the field of oncology are clearly structured and aim to control disease, reduce symptoms and improve long-term outcomes for patients’ health. Current information about NET treatment in Germany confirms that tactics are always selected individually, taking into account available services.
Surgical Treatment
Surgery remains the main method for many patients, especially in the early stages. With well-differentiated tumors, complete removal can be radical. The scope of the intervention varies from minimally invasive techniques to extended resections – depending on the spread of the process. Even with a metastatic course, cytoreductive surgery is sometimes performed to reduce tumor mass and improve the quality of life. For small formations of the appendix, small intestine or pancreas, surgery often has healing potential.
Radiation Therapy
Standard radiation therapy is of limited use in well-differentiated forms, as they are less sensitive to irradiation. At the same time, with aggressive neuroendocrine carcinomas or to control local symptoms (pain, bleeding), it can be an effective part of complex treatment.
Chemotherapy
Systemic medicine in the form of chemotherapy is usually used in low-differentiated or rapidly progressing forms. In certain cases of advanced well-differentiated tumors, this method is also considered, especially if other therapy options have failed.
Modern and Innovative Approaches to the Treatment of Neuroendocrine Tumors
In complex or advanced cases, standard therapy may not be sufficient. That is why innovative methods are actively implemented in Germany's healthcare system, which open up new opportunities for patients when traditional approaches have been exhausted. Current clinical information confirms the effectiveness of such strategies in specialized centers.
Peptide Receptor Radionuclide Therapy (PRRT)
Peptide receptor radionuclide therapy (PRRT) is one of the most promising methods for patients with highly differentiated metastatic tumors. The method involves delivering the isotope Lutetium-177 directly to cells expressing somatostatin receptors.
Unlike standard irradiation, the radioisotope acts in a targeted manner on tumor tissue, minimizing damage to healthy cells. PRRT can reduce tumor size, control symptoms, and contain progression over time. In a specialized hospital, treatment is carried out in accordance with international safety standards, which is especially important for patients with inoperable forms.
PRRT eligibility depends on confirmed somatostatin receptor expression — typically established through Ga-68 DOTATATE PET-CT.
A patient referred for Lutetium-177 therapy without that imaging has not yet been confirmed eligible for the treatment that motivated the referral.
Booking Health identifies whether somatostatin receptor scintigraphy has been performed and, where it has not, arranges the relevant PET-CT in Germany as the first step of the diagnostic-to-treatment sequence — so the PRRT program begins from a confirmed rather than presumed eligibility basis.
GET A SECOND OPINION FOR MY CASE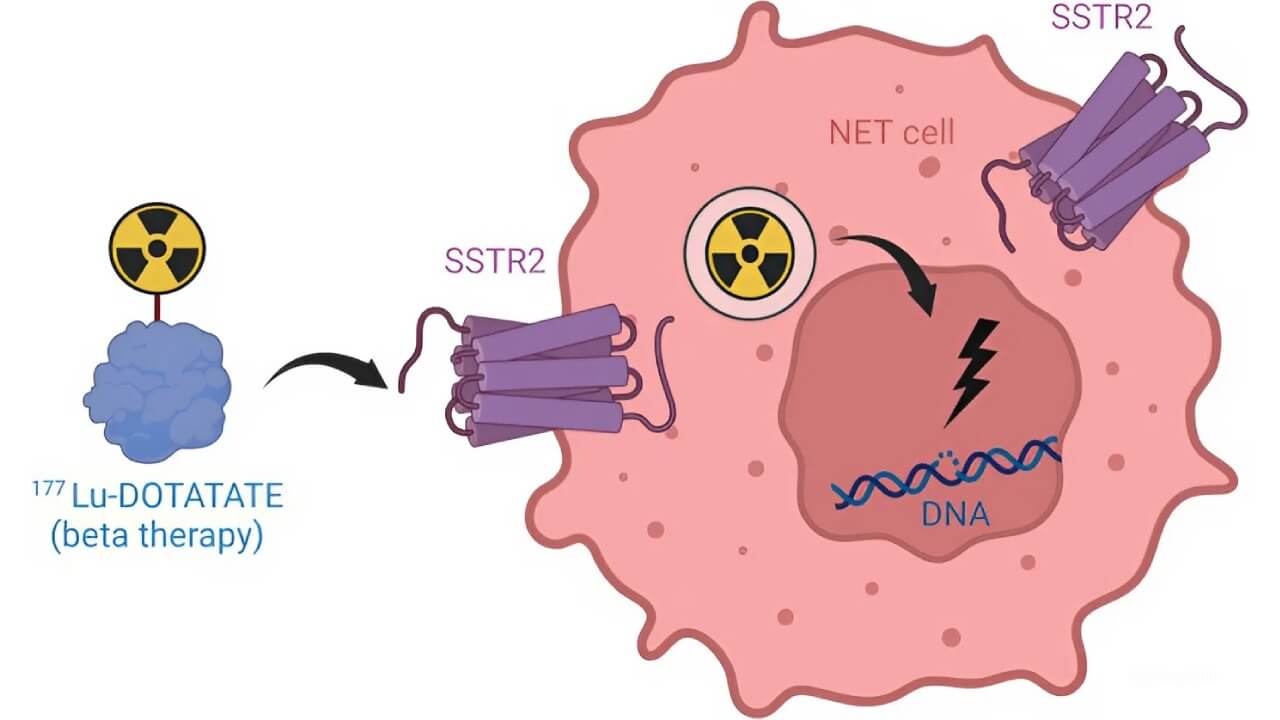
Transarterial Chemoembolization (TACE)
Transarterial chemoembolization, or TACE, is used mainly for liver metastases. During the procedure, the chemotherapy drug is injected directly into the arteries that feed the tumor, after which vascular embolization is performed. This allows doctors to keep the drug in the affected area and block the blood supply to the tumor.
This local approach ensures a high concentration of treatment in the desired area with fewer systemic side effects. In German interventional radiology centers, TACE is performed using modern imaging systems, which increases the safety of the procedure [9].

EXPERT
Professor Attila Kovács
Professor Kovács has over 26 years of experience in minimally invasive therapy. He specializes in transarterial chemoembolization (TACE) – a precise technique that delivers chemotherapy directly to tumors.
BOOK CONSULTATIONDendritic Cell Immunotherapy for Neuroendocrine Tumors
Unlike conventional treatments that target the tumor directly, dendritic cell therapy works by rebooting the immune system to do the job itself. It starts by collecting a patient’s immune cells through a blood drawing. These cells are then exposed to tumor-specific antigens in a lab, trained to recognize the cancer, and finally injected back into the patient to trigger a targeted immune attack [8].
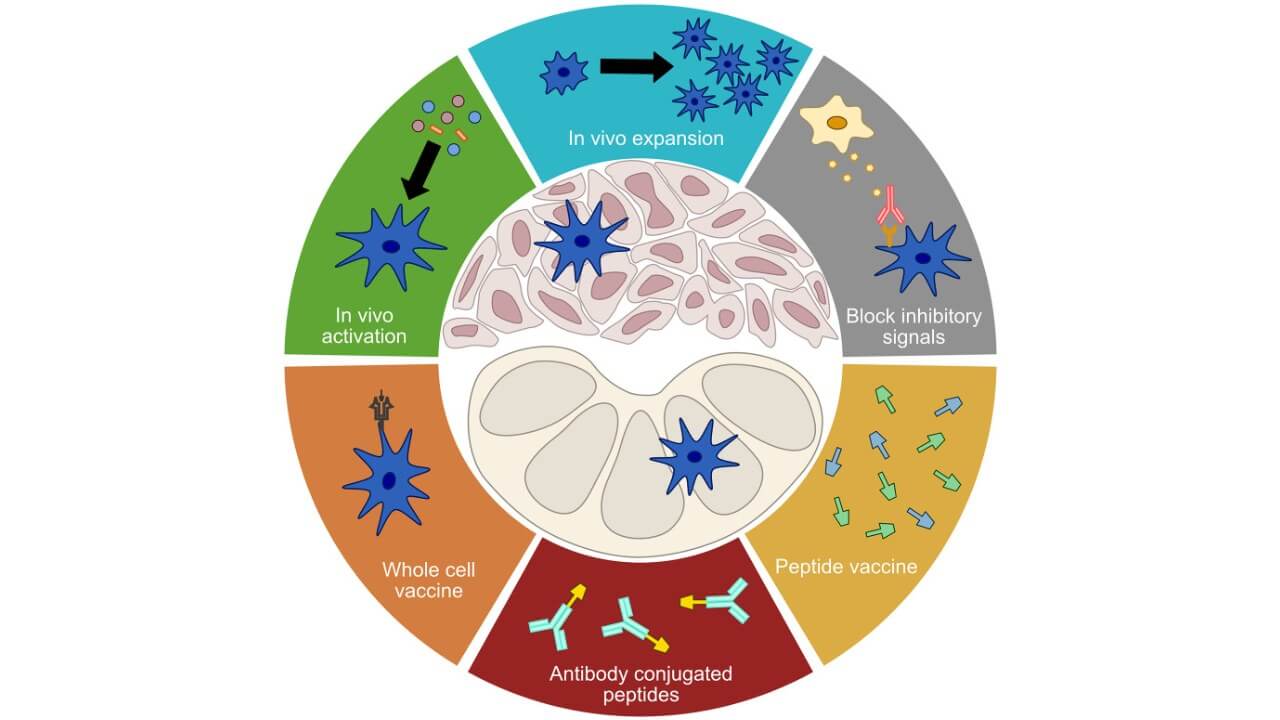
What makes this therapy so unique is its scientific foundation. Dendritic cells are the body’s key messengers between innate and adaptive immunity – something that wasn’t fully understood until their discovery fundamentally reshaped cancer immunology. That breakthrough earned global recognition in 2011, when Ralph Steinman’s work on dendritic cells was honored with the Nobel Prize [6].
In clinical practice, this approach has shown real-world benefits for patients with advanced or refractory neuroendocrine tumors: fewer side effects, better tolerance, and in many cases, meaningful tumor stabilization.
Comparative Table: NETs Treatments
Based on Booking Health clinical data and published outcomes. Actual results may vary depending on patient condition and treatment protocol.
| Therapy Type | 2-Year Survival Rate | Response Rate | Duration | Side Effects |
|---|---|---|---|---|
| Standard Treatments | ~55-70% for early stages ~30% for advanced stages | ~40-60% | Several weeks to months | Moderate to severe (fatigue, nausea, infertility, bowel/bladder issues) |
| Innovative Methods | ~60-75% in select advanced/refractory cases | 45-65% | Multiple sessions are possible | Mild (fever, localized inflammation, flu-like symptoms) |
"Select advanced/refractory cases" in the innovative methods row is the qualifier that determines whether a specific patient's outcome falls within that range.
For NETs, the selection variable is primarily somatostatin receptor expression level and Ki-67 index — patients with high receptor expression and low Ki-67 respond differently to PRRT than to DC vaccination, and the right innovative method depends on that distinction.
Booking Health's physician-level case review makes that determination within 24 hours of receiving the patient's diagnostic record.
Treatment of Neuroendocrine Tumors in Germany
Germany has an international reputation for high standards in oncology, particularly in the management of complex and rare pathologies such as neuroendocrine tumors. Thanks to modern diagnostics, a multidisciplinary approach and wide therapeutic possibilities, patients from different countries choose German clinics to receive accurate and personalized treatment.
Why Patients Choose Germany
One of the key advantages is a high level of specialization. Many hospitals operate within certified cancer networks, where surgeons, radiologists, endocrinologists, and nuclear medicine professionals collaborate as a single team. They have experience in the treatment of neuroendocrine tumors at all stages – from localized forms to metastatic ones.
Modern imaging methods and advanced hormone testing provide accurate diagnosis and staging, which allows doctors to form individual treatment plans using surgery, radiation therapy, Lutetium-based therapy, or immunotherapy.
With the support of the coordinated Booking Health system, foreign patients can access this level of medical care without organizational difficulties.
Leading Clinics and Oncology Centers
Numerous medical centers in Germany have international recognition in the field of treatment of neuroendocrine tumors. Continuity of care is a major strength: patients are followed closely by their medical team throughout every stage – from first consultation through treatment and aftercare.
Cost and Organization of Neuroendocrine Tumors Treatment in Germany
When it comes to neuroendocrine tumor treatment in Germany, costs are transparent and fixed by law. Patients receive detailed estimates covering everything from diagnostics and treatment to follow-up care. For international patients, Booking Health handles the full organization – from medical document review and hospital selection to appointment scheduling, translation, and cost control. This allows patients to focus on their recovery while all logistics and communication with German clinics are professionally managed.
Medical Procedures Costs for NETS
| Cost of treatment | Standard Methods | Innovative Methods |
|---|---|---|
| Price of Treatment in Germany | $25,000 – $280,000 for a full course | $6,500 – $38,000 for full course |
| Price of Treatment in the UK | $26,000 – $320,000 for a full course | $25,000 – $60,000 for a full course |
| Price of Treatment in the USA | $100,000 – $350,000 for a full course | $40,000 – $150,000 for a full course |
Germany's innovative method pricing represents the most accessible entry point globally for PRRT and DC vaccination combined.
Patients coordinating through Booking Health reach those rates without the foreign patient surcharge, receive a fully itemized budget before any commitment, and are covered by complication insurance of up to €200,000 as standard.
BOOK CONSULTATIONFrom Misdiagnosis To Clarity: How Maria Found Real Neuroendocrine Tumor Treatment Abroad
When Maria Estévez, a 46-year-old architect from Seville, started having episodes of facial flushing, abdominal pain, and unexplained fatigue, doctors initially thought it was early menopause. "I was told it was hormonal, stress-related. Nothing serious," she recalls.
However, the symptoms did not disappear, on the contrary, they became more pronounced. Further examination showed the presence of a neuroendocrine tumor (NET) in the pancreas, and at that time, metastases had already been detected in the liver.
The family began to look for more comprehensive treatment approaches and turned their attention to the Booking Health – service, which helps patients organize a full cycle of medical care in Germany.
"I filled out the online form late at night", – recalls Javier. "The very next morning, I was contacted by a Booking Health representative. They organized a detailed review of Maria's case and recommended a leading oncology clinic in Munich that specializes in treating NET using Lutetium therapy and immunotherapy".
Two weeks later, Maria was already in Germany. Once the diagnosis was confirmed, doctors developed a personalized treatment plan that included PRRT with Lutetium-177, hormone suppressive therapy, and nutritional support.
All organizational matters – registration for consultations, paperwork, translation and even living near the hospital – were taken over by Booking Health. "We have never felt confused", – says Javier. "The team has always acted proactively".
After three courses of therapy, Maria's disease stabilized. Symptoms diminished, she returned to part-time work and once again experienced energy and clarity of thought.
Advanced Cancer Treatment: Patient Success Stories with Booking Health













A Medical Journey: Every Step of the Way With Booking Health
Finding the best treatment strategy for your clinical situation is a challenging task. Being already exhausted from multiple treatment sessions, having consulted numerous specialists, and having tried various therapeutic interventions, you may be lost in all the information given by the doctors. In such a situation, it is easy to choose a first-hand option or to follow standardized therapeutic protocols with a long list of adverse effects instead of selecting highly specialized innovative treatment options.
To make an informed choice and get a personalized cancer management plan, which will be tailored to your specific clinical situation, consult medical experts at Booking Health. Being at the forefront of offering the latest medical innovations for already 12 years, Booking Health possesses solid expertise in creating complex NET management programs in each individual case. As a reputable company, Booking Health offers personalized neuroendocrine tumor treatment plans with direct clinic booking and full support at every stage, from organizational processes to assistance during treatment.
We provide:
- Assessment and analysis of medical reports
- Development of the medical care program
- Selection of a suitable treatment location
- Preparation of medical documents and forwarding to a suitable clinic
- Preparatory consultations with clinicians for the development of medical care programs
- Expert advice during the hospital stay
- Follow-up care after the patient returns to their native country after completing the medical care program
- Taking care of formalities as part of the preparation for the medical care program
- Coordination and organization of the patient's stay in a foreign country
- Assistance with visas and tickets
- A personal coordinator and interpreter with 24/7 support
- Transparent budgeting with no hidden costs
Health is an invaluable aspect of our lives. Delegating management of something so fragile yet precious should be done only to experts with proven experience and a reputation. Booking Health is a trustworthy partner who assists you in pursuing stronger health and a better quality of life. Contact our medical consultant to learn more about the possibilities of personalized treatment with innovative methods for neuroendocrine tumors with leading specialists in this field.
Booking Health holds ISO 9001 quality certification, reflecting well-established processes and strict quality control at every stage of the treatment journey — not just at the initial consultation, but throughout.

FAQ: Neuroendocrine Tumors
Neuroendocrine tumors (NETs) are rare growths that start in hormone-producing cells. They can occur in the lungs, pancreas, intestines, or other organs and often grow slowly, sometimes without early symptoms.
The exact cause isn’t always clear, but genetic factors, certain syndromes, and chronic inflammation in the gut or pancreas can play a role in developing neuroendocrine tumors.
Yes, neuroendocrine tumors are malignant neoplasms. Some of them grow slowly and can have a relatively favorable course for a long time, while others are characterized by aggressiveness and rapid metastasis, in particular low-differentiated neuroendocrine carcinomas.
The diagnostic process includes laboratory tests, assessment of tumor markers, imaging methods (CT, MRI, PET-CT), and morphological confirmation by biopsy. In Germany, modern algorithms are used that allow doctors to accurately establish the type and stage of a tumor.
The clinical status depends on the localization and biological features of the neoplasm. The most common are hot flashes, diarrhea, abdominal pain, and unexplained weight loss. Hormonally active tumors can cause additional systemic symptoms..
Therapy is tailored and may include surgery, PRRT, TACE, or immunotherapy. Leading clinics in Germany offer comprehensive treatment programs taking into account the degree of malignancy and the spread of the process.
With early detection and radical surgical removal, neuroendocrine tumors can be cured. In the case of advanced forms, treatment in Germany is aimed at long-term disease control and maintaining the quality of life.
PRRT is a peptide-receptor radionuclide therapy that uses Lutetium-177 to target tumor cells. In Germany, it is conducted in specialized departments of nuclear medicine, and it demonstrates effectiveness in many forms of NETs.
Immunotherapy, in particular with the use of dendritic cells, can be effective in certain clinical situations. In Germany, such approaches are implemented within personalized programs, especially when standard methods have limited effectiveness.
Top centers for neuroendocrine tumors in Germany include clinics in Munich, Heidelberg, and Essen. Many are part of certified oncology networks offering multidisciplinary care.
In Germany, standard treatment costs approximately $25,000-280,000 and innovative methods cost $6,500-38,000. In the UK, costs are $26,000-320,000 and $25,000-60,000 respectively. In the US, these amounts can reach $100,000-350,000 and $40,000-150,000. In Australia, access to modern methods is often limited, and prices are sometimes several times higher than European prices.
NETs are treated by a team of specialists: oncologists, surgeons, endocrinologists, and nuclear medicine experts – especially in dedicated NET clinics in Germany.
Yes, many German hospitals offer expert second opinions. Booking Health can arrange case reviews by NET specialists, even before you travel, based on your existing medical documents.
You can contact Booking Health to coordinate every step - from medical record review and clinic selection to visa support and translation - ensuring smooth access to NET treatment in Germany.
Neuroendocrine tumor therapy may include surgery, chemotherapy, and modern methods, including PRRT, TACE, and dendritic cell immunotherapy. The choice of tactics is determined by the stage, localization and degree of malignancy of the tumor.
Manifestations depend on the location of the tumor and its hormonal activity. Typical symptoms include abdominal pain, diarrhea, flushing, wheezing, weakness, and unexplained weight loss. Hormonally active forms can cause carcinoid syndrome with flushing and damage to heart valves.
In Germany, standard neuroendocrine tumor (NET) treatment costs range from $25,000-$280,000, and innovative methods cost $6,500-$38,000. In the UK, prices range from $26,000-$320,000 and $25,000-$60,000, while in the USA, they reach $100,000-$350,000 and $40,000-$150,000, respectively. In contrast, Australia often has limited access to advanced NET therapies, and prices can be up to four times higher than in Europe.
With standard treatment, the rate is about 55-70%. Applying innovative methods such as PRRT, TACE or immunotherapy can increase it by up to 60-75%, especially in complex or advanced cases.
Treatment efficacy varies, with standard approaches showing response in 40-60% of cases, while current methods, including PRRT and dendritic cell therapy, in approximately 45-65%, providing better disease control.
Traditional methods can cause fatigue, nausea, indigestion, skin irritation, or fertility effects. Innovative approaches usually have a milder safety profile and can cause mild flu-like symptoms or local reactions.
Standard therapy usually takes several weeks to several months. Innovative methods, particularly PRRT or dendritic cell vaccination, are conducted in courses of several sessions in a relatively short period, which may contribute to faster recovery and improved quality of life.
Choose treatment abroad and you will be sure to get the best results!
Sources:
01. Peiwen Wu, Dongjie He, Hao Chang, Xiaozhi Zhang. Epidemiologic trends of and factors associated with overall survival in patients with neuroendocrine tumors over the last two decades in the USA. Endocr Connect. 2023 Nov 23;12(12):e230331. doi: 10.1530/EC-23-0331. [DOI] [PMC free article]
02. Qamar Sultana, Jill Kar, Amogh Verma at al. A Comprehensive Review on Neuroendocrine Neoplasms: Presentation, Pathophysiology and Management. J Clin Med. 2023 Aug 5;12(15):5138. doi: 10.3390/jcm12155138. [DOI] [PubMed]
03. Bryan Oronsky, Patrick C Ma, Daniel Morgensztern, Corey A Carter. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia . 2017 Dec;19(12):991-1002. doi: 10.1016/j.neo.2017.09.002. Epub 2017 Nov 5. [DOI] [PubMed]
04. Jessica E Maxwell, James R Howe. Imaging in neuroendocrine tumors: an update for the clinician. Int J Endocr Oncol. 2015;2(2):159-168. doi: 10.2217/ije.14.40. [DOI] [PubMed]
05. Jelka Kuiper, Eline Zoetelief, Tessa Brabander, Wouter W de Herder, Johannes Hofland. Current status of peptide receptor radionuclide therapy in grade 1 and 2 gastroenteropancreatic neuroendocrine tumours. J Neuroendocrinol. 2025 Mar;37(3):e13469. doi: 10.1111/jne.13469. Epub 2024 Nov 20. [DOI] [PubMed]
06. Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x. [DOI] [PubMed]
07. Alycia Gardner, Álvaro de Mingo Pulido, Brian Ruffell. Dendritic Cells and Their Role in Immunotherapy. Front Immunol. 2020 May 21;11:924. doi: 10.3389/fimmu.2020.00924. [DOI] [PMC free article]
08. Neale Hanke, Darya Alizadeh, Emmanuel Katsanis, Nicolas Larmonier. Dendritic cell tumor killing activity and its potential applications in cancer immunotherapy. Crit Rev Immunol. 2013;33(1):1–21. doi: 10.1615/critrevimmunol.2013006679. [DOI] [PMC free article]
09. Hu Xu, Li Zhang, Juan Zhang et al. Efficacy of transcatheter arterial chemoembolization-based multimodal treatment in patients with neuroendocrine tumors involving the liver. Transl Cancer Res. 2025 Jul 17;14(7):4321–4330. doi: 10.21037/tcr-2024-2482. [DOI] [PMC free article]
10. Paweł Gut, Agata Czarnywojtek, Jakub Fischbach et al. Chromogranin A – unspecific neuroendocrine marker. Clinical utility and potential diagnostic pitfalls. Arch Med Sci. 2016 Feb 2;12(1):1–9. doi: 10.5114/aoms.2016.57577. [DOI] [PMC free article]
Read:
01. New Effective Treatments for Stage 4 Cancer: Innovations in Oncology
02. Treatment of Gastrointestinal Neuroendocrine Tumors
03. Gastrointestinal oncology in the fight against cancer: meeting with experts